

Estimating the health burden of road traffic injuries in Malawi using an individual-based model
- PMID: 35821170
- PMCID: PMC9275162
- DOI: 10.1186/s40621-022-00386-6
Estimating the health burden of road traffic injuries in Malawi using an individual-based model
Abstract
Background: Road traffic injuries are a significant cause of death and disability globally. However, in some countries the exact health burden caused by road traffic injuries is unknown. In Malawi, there is no central reporting mechanism for road traffic injuries and so the exact extent of the health burden caused by road traffic injuries is hard to determine. A limited number of models predict the incidence of mortality due to road traffic injury in Malawi. These estimates vary greatly, owing to differences in assumptions, and so the health burden caused on the population by road traffic injuries remains unclear.
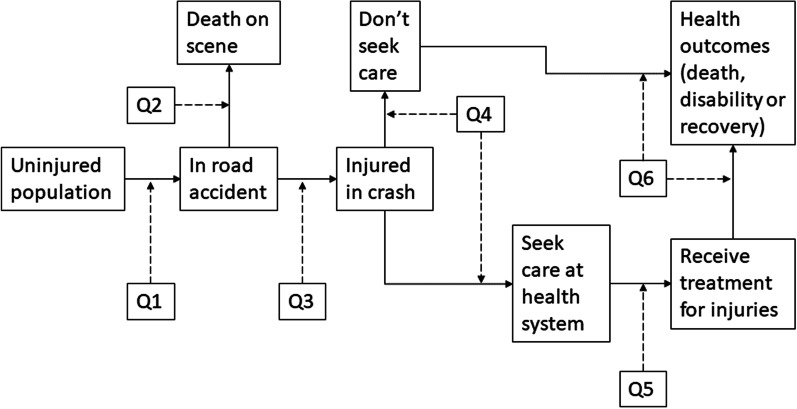
Methods: We use an individual-based model and combine an epidemiological model of road traffic injuries with a health seeking behaviour and health system model. We provide a detailed representation of road traffic injuries in Malawi, from the onset of the injury through to the final health outcome. We also investigate the effects of an assumption made by other models that multiple injuries do not contribute to health burden caused by road accidents.
Results: Our model estimates an overall average incidence of mortality between 23.5 and 29.8 per 100,000 person years due to road traffic injuries and an average of 180,000 to 225,000 disability-adjusted life years (DALYs) per year between 2010 and 2020 in an estimated average population size of 1,364,000 over the 10-year period. Our estimated incidence of mortality falls within the range of other estimates currently available for Malawi, whereas our estimated number of DALYs is greater than the only other estimate available for Malawi, the GBD estimate predicting and average of 126,200 DALYs per year over the same time period. Our estimates, which account for multiple injuries, predict a 22-58% increase in overall health burden compared to the model ran as a single injury model.
Conclusions: Road traffic injuries are difficult to model with conventional modelling methods, owing to the numerous types of injuries that occur. Using an individual-based model framework, we can provide a detailed representation of road traffic injuries. Our results indicate a higher health burden caused by road traffic injuries than previously estimated.
Keywords: Health burden; Individual-based model; Malawi; Road traffic injuries.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that we have no competing interests.
Figures






References
-
- Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, Abdollahpour I, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi: 10.1016/S0140-6736(20)30925-9/ATTACHMENT/96EE692B-E8A2-4D2B-AB04-5A9B1490A107/MMC2E.PDF. - DOI - PMC - PubMed
-
- Akinpelu OV, Oladele OA, Amusa YB, Ogundipe OK, Adeolu AA, Komolafe EO. Review of road traffic accident admissions in a Nigerian Tertiary Hospital. Revi Road Traffic Acc Admin Nigeri Tertiary Hosp. 2007;12(1):63–67.
-
- Banza LN, Gallaher J, Dybvik E, Charles A, Hallan G, Gjertsen J-E, Mkandawire N, Varela C, Young S. The rise in road traffic injuries in Lilongwe, Malawi a snapshot of the growing epidemic of trauma in low income countries. Int J Surg Open. 2018;10:55–60. doi: 10.1016/j.ijso.2017.11.004. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
