

Multi-center validation of machine learning model for preoperative prediction of postoperative mortality
- PMID: 35821515
- PMCID: PMC9276734
- DOI: 10.1038/s41746-022-00625-6
Multi-center validation of machine learning model for preoperative prediction of postoperative mortality
Abstract
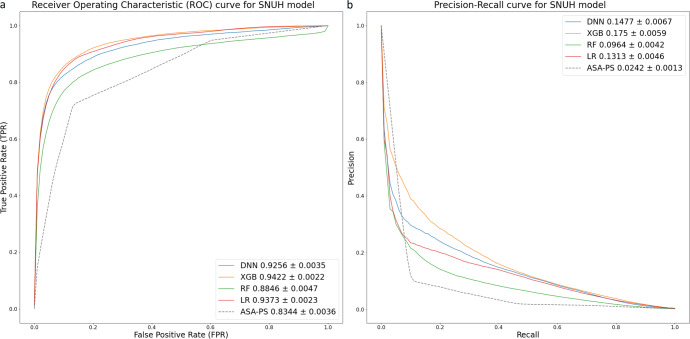
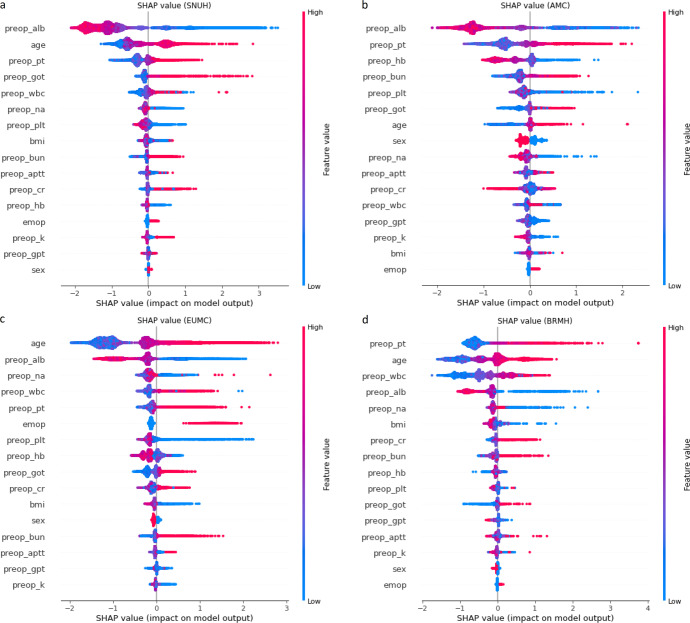
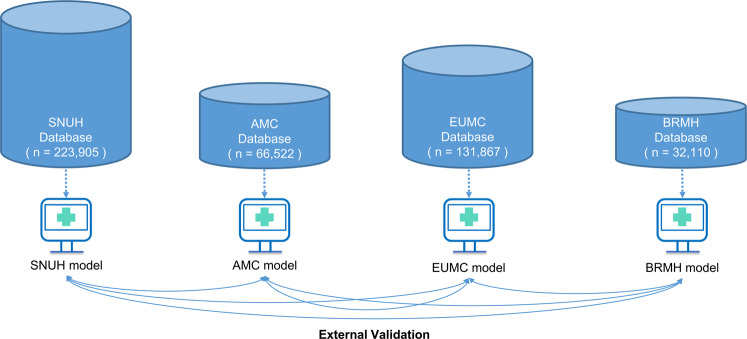
Accurate prediction of postoperative mortality is important for not only successful postoperative patient care but also for information-based shared decision-making with patients and efficient allocation of medical resources. This study aimed to create a machine-learning prediction model for 30-day mortality after a non-cardiac surgery that adapts to the manageable amount of clinical information as input features and is validated against multi-centered rather than single-centered data. Data were collected from 454,404 patients over 18 years of age who underwent non-cardiac surgeries from four independent institutions. We performed a retrospective analysis of the retrieved data. Only 12-18 clinical variables were used for model training. Logistic regression, random forest classifier, extreme gradient boosting (XGBoost), and deep neural network methods were applied to compare the prediction performances. To reduce overfitting and create a robust model, bootstrapping and grid search with tenfold cross-validation were performed. The XGBoost method in Seoul National University Hospital (SNUH) data delivers the best performance in terms of the area under receiver operating characteristic curve (AUROC) (0.9376) and the area under the precision-recall curve (0.1593). The predictive performance was the best when the SNUH model was validated with Ewha Womans University Medical Center data (AUROC, 0.941). Preoperative albumin, prothrombin time, and age were the most important features in the model for each hospital. It is possible to create a robust artificial intelligence prediction model applicable to multiple institutions through a light predictive model using only minimal preoperative information that can be automatically extracted from each hospital.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Weiser TG, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015;385:S11. - PubMed
-
- Stephenson C, et al. Management of common postoperative complications. Mayo Clin. Proc. 2020;95:2540–2554. - PubMed
-
- Anderson O, Davis R, Hanna GB, Vincent CA. Surgical adverse events: a systematic review. Am. J. Surg. 2013;206:253–262. - PubMed
-
- Brennan TA, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical practice study I. N. Engl. J. Med. 1991;324:370–376. - PubMed
LinkOut - more resources
Full Text Sources
