

Post-vaccination infection rates and modification of COVID-19 symptoms in vaccinated UK school-aged children and adolescents: A prospective longitudinal cohort study
- PMID: 35821715
- PMCID: PMC9263281
- DOI: 10.1016/j.lanepe.2022.100429
Post-vaccination infection rates and modification of COVID-19 symptoms in vaccinated UK school-aged children and adolescents: A prospective longitudinal cohort study
Abstract
Background: We aimed to explore the effectiveness of one-dose BNT162b2 vaccination upon SARS-CoV-2 infection, its effect on COVID-19 presentation, and post-vaccination symptoms in children and adolescents (CA) in the UK during periods of Delta and Omicron variant predominance.
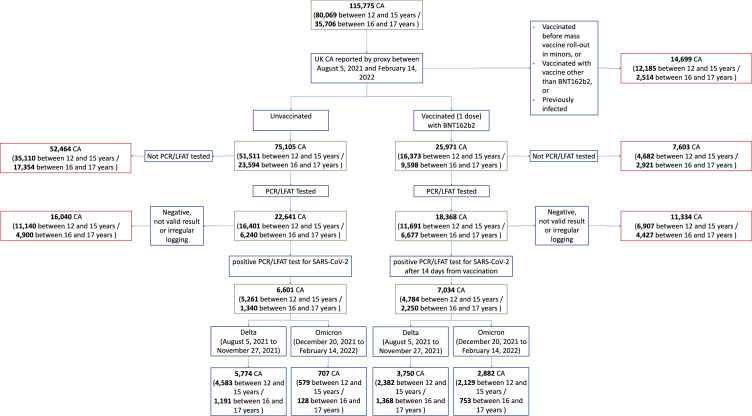
Methods: In this prospective longitudinal cohort study, we analysed data from 115,775 CA aged 12-17 years, proxy-reported through the Covid Symptom Study (CSS) smartphone application. We calculated post-vaccination infection risk after one dose of BNT162b2, and described the illness profile of CA with post-vaccination SARS-CoV-2 infection, compared to unvaccinated CA, and post-vaccination side-effects.
Findings: Between August 5, 2021 and February 14, 2022, 25,971 UK CA aged 12-17 years received one dose of BNT162b2 vaccine. The probability of testing positive for infection diverged soon after vaccination, and was lower in CA with prior SARS-CoV-2 infection. Vaccination reduced proxy-reported infection risk (-80·4% (95% CI -0·82 -0·78) and -53·7% (95% CI -0·62 -0·43) at 14-30 days with Delta and Omicron variants respectively, and -61·5% (95% CI -0·74 -0·44) and -63·7% (95% CI -0·68 -0.59) after 61-90 days). Vaccinated CA who contracted SARS-CoV-2 during the Delta period had milder disease than unvaccinated CA; during the Omicron period this was only evident in children aged 12-15 years. Overall disease profile was similar in both vaccinated and unvaccinated CA. Post-vaccination local side-effects were common, systemic side-effects were uncommon, and both resolved within few days (3 days in most cases).
Interpretation: One dose of BNT162b2 vaccine reduced risk of SARS-CoV-2 infection for at least 90 days in CA aged 12-17 years. Vaccine protection varied for SARS-CoV-2 variant type (lower for Omicron than Delta variant), and was enhanced by pre-vaccination SARS-CoV-2 infection. Severity of COVID-19 presentation after vaccination was generally milder, although unvaccinated CA also had generally mild disease. Overall, vaccination was well-tolerated.
Funding: UK Government Department of Health and Social Care, Chronic Disease Research Foundation, The Wellcome Trust, UK Engineering and Physical Sciences Research Council, UK Research and Innovation London Medical Imaging & Artificial Intelligence Centre for Value Based Healthcare, UK National Institute for Health Research, UK Medical Research Council, British Heart Foundation and Alzheimer's Society, and ZOE Limited.
Keywords: BNT162b2 vaccine effectiveness; BNT162b2, Comirnaty SARS-CoV-2 vaccine (BioNTech, Pfizer); CA, Children and adolescents; COVID-19 vaccination; KCL, King's College London; LFAT, Lateral flow antigen test; OR, Odds Ratio; PCR, Polymerase chain reaction; Paediatrics; SARS-CoV-2 vaccination; SARS-CoV-2 vaccination in children; SARS-CoV-2, Severe acute respiratory syndrome‐related coronavirus 2; UK, United Kingdom of Great Britain and Northern Ireland.
© 2022 The Author(s).
Conflict of interest statement
JCP, LP, AM, JW are employees of Zoe Limited. TDS and SO report being consultants for Zoe Limited, during the conduct of the study. All other authors have nothing to declare.
Figures





References
-
- Stephenson T, Pinto Pereira SM, Shafran R, et al. Physical and mental health 3 months after SARS-CoV-2 infection (long COVID) among adolescents in England (CLoCk): a national matched cohort study. Lancet Child Adolesc Health. 2022 doi: 10.1016/S2352-4642(22)00022-0. published online Feb. - DOI - PMC - PubMed
-
- Naleway AL, Groom HC, Crawford PM, et al. Incidence of SARS-CoV-2 Infection, Emergency Department Visits, and Hospitalizations Because of COVID-19 Among Persons Aged ≥12 Years, by COVID-19 Vaccination Status — Oregon and Washington, July 4–September 25, 2021. MMWR Morb Mortal Wkly Rep. 2021;70 doi: 10.15585/mmwr.mm7046a4. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
