

Stem Cells in the Myelodysplastic Syndromes
- PMID: 35822030
- PMCID: PMC9261372
- DOI: 10.3389/fragi.2021.719010
Stem Cells in the Myelodysplastic Syndromes
Abstract
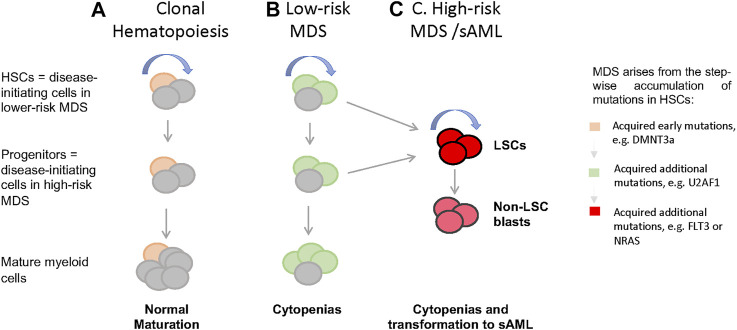
The myelodysplastic syndromes (MDS) represent a group of clonal disorders characterized by ineffective hematopoiesis, resulting in peripheral cytopenias and frequent transformation to acute myeloid leukemia (AML). We and others have demonstrated that MDS arises in, and is propagated by malignant stem cells (MDS-SCs), that arise due to the sequential acquisition of genetic and epigenetic alterations in normal hematopoietic stem cells (HSCs). This review focuses on recent advancements in the cellular and molecular characterization of MDS-SCs, as well as their role in mediating MDS clinical outcomes. In addition to discussing the cell surface proteins aberrantly upregulated on MDS-SCs that have allowed the identification and prospective isolation of MDS-SCs, we will discuss the recurrent cytogenetic abnormalities and genetic mutations present in MDS-SCs and their roles in initiating disease, including recent studies demonstrating patterns of clonal evolution and disease progression from pre-malignant HSCs to MDS-SCs. We also will discuss the pathways that have been described as drivers or promoters of disease, including hyperactivated innate immune signaling, and how the identification of these alterations in MDS-SC have led to investigations of novel therapeutic strategies to treat MDS. It is important to note that despite our increasing understanding of the pathogenesis of MDS, the molecular mechanisms that drive responses to therapy remain poorly understood, especially the mechanisms that underlie and distinguish hematologic improvement from reductions in blast burden. Ultimately, such distinctions will be required in order to determine the shared and/or unique molecular mechanisms that drive ineffective hematopoiesis, MDS-SC maintenance, and leukemic transformation.
Keywords: acute myeloid leukemia; clonal hematopoiesis; hematopoietic stem cells; myelodysplastic syndromes; novel therapeutics.
Copyright © 2021 Zhan and Park.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Stem Cells in Myelodysplastic Syndromes and Acute Myeloid Leukemia: First Cousins or Unrelated Entities?Front Oncol. 2021 Aug 20;11:730899. doi: 10.3389/fonc.2021.730899. eCollection 2021. Front Oncol. 2021. PMID: 34490124 Free PMC article. Review.
-
Targeting stem cells in myelodysplastic syndromes and acute myeloid leukemia.J Intern Med. 2022 Aug;292(2):262-277. doi: 10.1111/joim.13535. Epub 2022 Jul 13. J Intern Med. 2022. PMID: 35822488 Free PMC article. Review.
-
Myelodysplastic syndrome hematopoietic stem cell.Int J Cancer. 2013 Aug 1;133(3):525-33. doi: 10.1002/ijc.27896. Epub 2012 Oct 29. Int J Cancer. 2013. PMID: 23047726 Review.
-
[Senescent Mesenchymal Stem Cells Contribute to Progression of Myelodysplastic Syndromes-Review].Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2018 Jun;26(3):942-946. doi: 10.7534/j.issn.1009-2137.2018.03.053. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2018. PMID: 29950248 Review. Chinese.
-
Physician Education: Myelodysplastic Syndrome.Oncologist. 1996;1(4):284-287. Oncologist. 1996. PMID: 10388004
Cited by
-
Molecular Targeted Therapy and Immunotherapy for Myelodysplastic Syndrome.Int J Mol Sci. 2021 Sep 23;22(19):10232. doi: 10.3390/ijms221910232. Int J Mol Sci. 2021. PMID: 34638574 Free PMC article. Review.
-
Single-cell transcriptomics dissects the transcriptome alterations of hematopoietic stem cells in myelodysplastic neoplasms.J Transl Med. 2024 Apr 17;22(1):359. doi: 10.1186/s12967-024-05165-z. J Transl Med. 2024. PMID: 38632656 Free PMC article.
-
Why Single-Cell Sequencing Has Promise in MDS.Front Oncol. 2021 Dec 2;11:769753. doi: 10.3389/fonc.2021.769753. eCollection 2021. Front Oncol. 2021. PMID: 34926276 Free PMC article. Review.
-
SMC2 and Condensin II Subunits Are Essential for the Development of Hematopoietic Stem and Progenitor Cells in Zebrafish.J Cell Physiol. 2025 Mar;240(3):e70023. doi: 10.1002/jcp.70023. J Cell Physiol. 2025. PMID: 40134128 Free PMC article.
-
NF-κB and Pancreatic Cancer; Chapter and Verse.Cancers (Basel). 2021 Sep 7;13(18):4510. doi: 10.3390/cancers13184510. Cancers (Basel). 2021. PMID: 34572737 Free PMC article. Review.
References
-
- Allampallam K., Shetty V., Mundle S., Dutt D., Kravitz H., Reddy P. L., et al. (2002). Biological Significance of Proliferation, Apoptosis, Cytokines, and Monocyte/macrophage Cells in Bone Marrow Biopsies of 145 Patients with Myelodysplastic Syndrome. Int. J. Hematol. 75 (3), 289–297. 10.1007/bf02982044 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous