

Efficacy and safety of oral semaglutide in patients with non-alcoholic fatty liver disease complicated by type 2 diabetes mellitus: A pilot study
- PMID: 35822119
- PMCID: PMC9260206
- DOI: 10.1002/jgh3.12780
Efficacy and safety of oral semaglutide in patients with non-alcoholic fatty liver disease complicated by type 2 diabetes mellitus: A pilot study
Abstract
Background and aim: This study aimed to clarify the efficacy and safety of oral semaglutide treatment in patients with non-alcoholic fatty liver disease (NAFLD) complicated by type 2 diabetes mellitus (T2DM).
Methods: This was a single-arm, open-label pilot study. Sixteen patients with NAFLD who received oral semaglutide for T2DM were included in the analysis. Oral semaglutide was initiated at a dose of 3 mg once daily, and the dose was sequentially increased to 7 mg at 4 weeks and 14 mg at 8 weeks (maintenance dose) until the end of the 24-week trial.
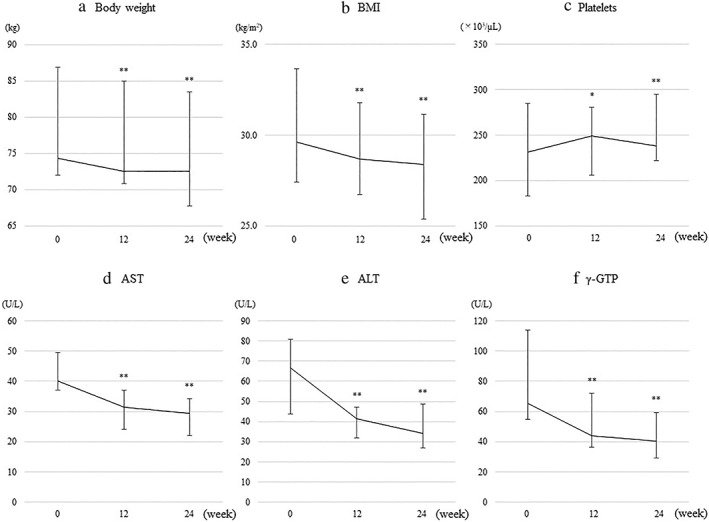
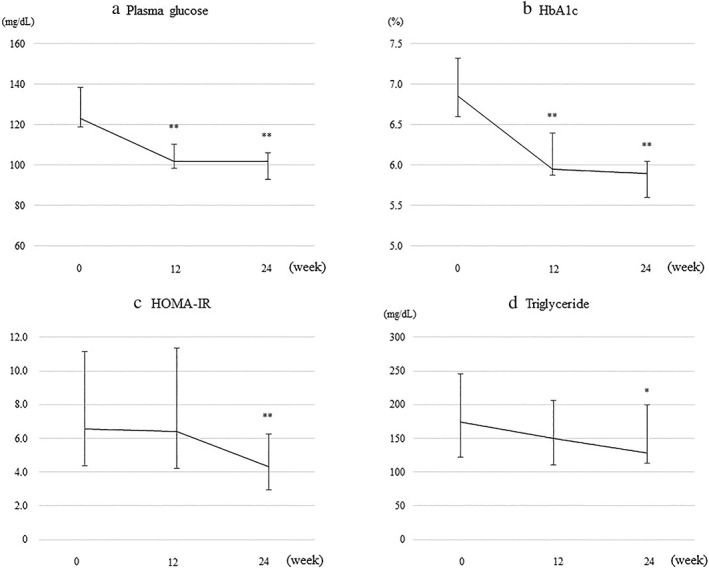
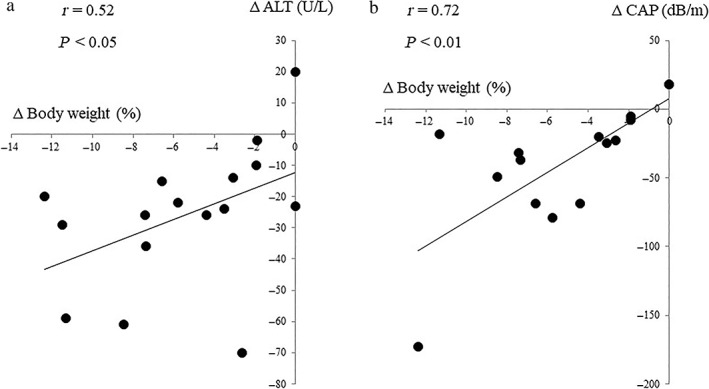
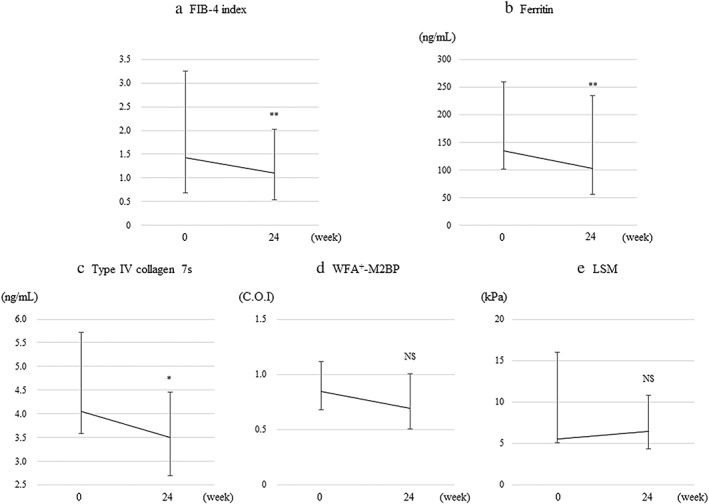
Results: Body weight and levels of liver-related biochemistry, plasma glucose, and hemoglobin A1c decreased significantly from baseline to 12 weeks. These significant decreases were maintained until the end of the trial. Additionally, levels of the homeostasis model assessment-insulin resistance and triglyceride significantly decreased at 24 weeks. Controlled attenuation parameter (CAP) values significantly decreased from baseline to 24 weeks. Changes in body weight were correlated with those in levels of alanine aminotransferase (r = 0.52) and CAP (r = 0.72). As for liver fibrosis markers, significant decreases from baseline to 24 weeks in levels of the fibrosis-4 index, ferritin, and type IV collagen 7 s were found; however, the liver stiffness measurement did not significantly decrease. Most adverse events were grade 1-2 transient gastrointestinal disorders.
Conclusions: Oral semaglutide treatment in patients with NAFLD complicated by T2DM improved impaired liver function, hypertriglyceridemia, insulin resistance, and hepatic steatosis, as well as improving diabetic status and reducing body weight.
Keywords: GLP‐1 receptor agonists; controlled attenuation parameter; liver fibrosis; non‐alcoholic fatty liver disease; semaglutide.
© 2022 The Authors. JGH Open published by Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Figures
References
-
- Younossi Z, Anstee QM, Marietti M et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018; 15: 1120. - PubMed
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease‐meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016; 64: 73–84. - PubMed
-
- Farrell GC, Wong VW, Chitturi S. NAFLD in Asia—as common and important as in the West. Nat. Rev. Gastroenterol. Hepatol. 2013; 10: 307–18. - PubMed
-
- Farrell GC, Larter CZ. Nonalcoholic fatty liver disease: from steatosis to cirrhosis. Hepatology. 2006; 43: S99–S112. - PubMed
-
- Lonardo A, Nascimbeni F, Targher G et al. AISF position paper on nonalcoholic fatty liver disease (NAFLD): updates and future directions. Dig. Liver Dis. 2017; 49: 471–83. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
