

Targeting stem cells in myelodysplastic syndromes and acute myeloid leukemia
- PMID: 35822488
- PMCID: PMC9544124
- DOI: 10.1111/joim.13535
Targeting stem cells in myelodysplastic syndromes and acute myeloid leukemia
Abstract
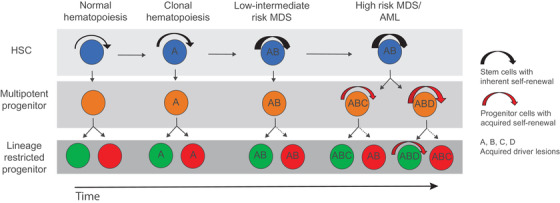
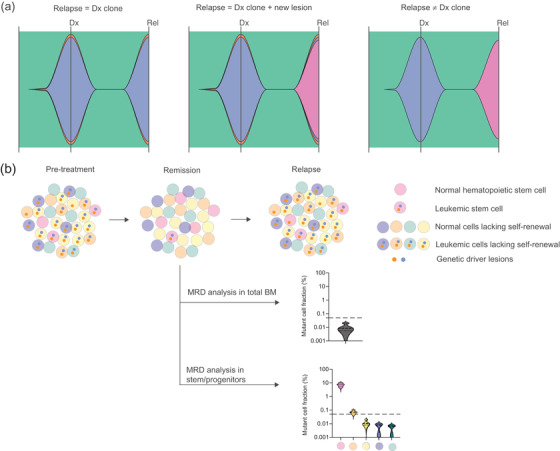
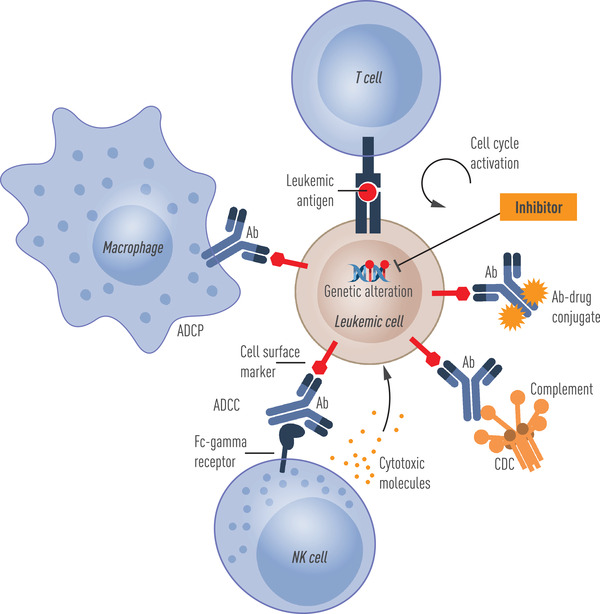
The genetic architecture of cancer has been delineated through advances in high-throughput next-generation sequencing, where the sequential acquisition of recurrent driver mutations initially targeted towards normal cells ultimately leads to malignant transformation. Myelodysplastic syndromes (MDS) and acute myeloid leukemia (AML) are hematologic malignancies frequently initiated by mutations in the normal hematopoietic stem cell compartment leading to the establishment of leukemic stem cells. Although the genetic characterization of MDS and AML has led to identification of new therapeutic targets and development of new promising therapeutic strategies, disease progression, relapse, and treatment-related mortality remain a major challenge in MDS and AML. The selective persistence of rare leukemic stem cells following therapy-induced remission implies unique resistance mechanisms of leukemic stem cells towards conventional therapeutic strategies and that leukemic stem cells represent the cellular origin of relapse. Therefore, targeted surveillance of leukemic stem cells following therapy should, in the future, allow better prediction of relapse and disease progression, but is currently challenged by our restricted ability to distinguish leukemic stem cells from other leukemic cells and residual normal cells. To advance current and new clinical strategies for the treatment of MDS and AML, there is a need to improve our understanding and characterization of MDS and AML stem cells at the cellular, molecular, and genetic levels. Such work has already led to the identification of promising new candidate leukemic stem cell molecular targets that can now be exploited in preclinical and clinical therapeutic strategies, towards more efficient and specific elimination of leukemic stem cells.
Keywords: acute myeloid leukemia; clonal evolution; hematopoietic stem cells; leukemic stem cells; myelodysplastic syndromes; therapeutic targets.
© 2022 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
B. L. E. has received research funding from Celgene, Deerfield, Novartis, and Calico and consulting fees from GRAIL. B. L. E. is a member of the scientific advisory board and shareholder for Neomorph Therapeutics, TenSixteen Bio, Skyhawk Therapeutics, and Exo Therapeutics. T. F. is a cofounder and board member and owns shares in Cantargia AB. All the other authors have no conflict of interest to declare.
Figures
Similar articles
-
Myelodysplastic syndrome progression to acute myeloid leukemia at the stem cell level.Nat Med. 2019 Jan;25(1):103-110. doi: 10.1038/s41591-018-0267-4. Epub 2018 Dec 3. Nat Med. 2019. PMID: 30510255 Free PMC article.
-
Stem Cells in the Myelodysplastic Syndromes.Front Aging. 2021 Jul 16;2:719010. doi: 10.3389/fragi.2021.719010. eCollection 2021. Front Aging. 2021. PMID: 35822030 Free PMC article. Review.
-
Transformation of myelodysplastic syndromes into acute myeloid leukemias.Chin Med J (Engl). 2004 Jul;117(7):963-7. Chin Med J (Engl). 2004. PMID: 15265365
-
[Senescent Mesenchymal Stem Cells Contribute to Progression of Myelodysplastic Syndromes-Review].Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2018 Jun;26(3):942-946. doi: 10.7534/j.issn.1009-2137.2018.03.053. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2018. PMID: 29950248 Review. Chinese.
-
Stem Cells in Myelodysplastic Syndromes and Acute Myeloid Leukemia: First Cousins or Unrelated Entities?Front Oncol. 2021 Aug 20;11:730899. doi: 10.3389/fonc.2021.730899. eCollection 2021. Front Oncol. 2021. PMID: 34490124 Free PMC article. Review.
Cited by
-
Transcription elongation defects link oncogenic SF3B1 mutations to targetable alterations in chromatin landscape.Mol Cell. 2024 Apr 18;84(8):1475-1495.e18. doi: 10.1016/j.molcel.2024.02.032. Epub 2024 Mar 22. Mol Cell. 2024. PMID: 38521065 Free PMC article.
-
Phenolic Composition of Crataegus monogyna Jacq. Extract and Its Anti-Inflammatory, Hepatoprotective, and Antileukemia Effects.Pharmaceuticals (Basel). 2024 Jun 15;17(6):786. doi: 10.3390/ph17060786. Pharmaceuticals (Basel). 2024. PMID: 38931453 Free PMC article.
-
Sox13 and M2-like leukemia-associated macrophages contribute to endogenous IL-34 caused accelerated progression of acute myeloid leukemia.Cell Death Dis. 2023 May 6;14(5):308. doi: 10.1038/s41419-023-05822-z. Cell Death Dis. 2023. PMID: 37149693 Free PMC article.
-
Single-Cell Next-Generation Sequencing to Monitor Hematopoietic Stem-Cell Transplantation: Current Applications and Future Perspectives.Cancers (Basel). 2023 Apr 26;15(9):2477. doi: 10.3390/cancers15092477. Cancers (Basel). 2023. PMID: 37173944 Free PMC article. Review.
-
p53 biology and reactivation for improved therapy in MDS and AML.Biomark Res. 2024 Mar 13;12(1):34. doi: 10.1186/s40364-024-00579-9. Biomark Res. 2024. PMID: 38481290 Free PMC article. Review.
References
-
- Moscow JA, Fojo T, Schilsky RL. The evidence framework for precision cancer medicine. Nat Rev Clin Oncol. 2018;15(3):183–92. - PubMed
-
- Mateo J, Steuten L, Aftimos P, André F, Davies M, Garralda E, et al. Delivering precision oncology to patients with cancer. Nat Med. 2022;28(4):658–65. - PubMed
-
- Martínez‐Jiménez F, Muiños F, Sentís I, Deu‐Pons J, Reyes‐Salazar I, Arnedo‐Pac C, et al. A compendium of mutational cancer driver genes. Nat Rev Cancer. 2020;20(10):555–72. - PubMed
-
- Batlle E, Clevers H. Cancer stem cells revisited. Nat Med. 2017;23(10):1124–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
