

Critical Analysis and Limitations of the Diagnosis of Heart Failure with Preserved Ejection Fraction (HFpEF)
- PMID: 35830074
- PMCID: PMC9438546
- DOI: 10.36660/abc.20210052
Critical Analysis and Limitations of the Diagnosis of Heart Failure with Preserved Ejection Fraction (HFpEF)
Abstract
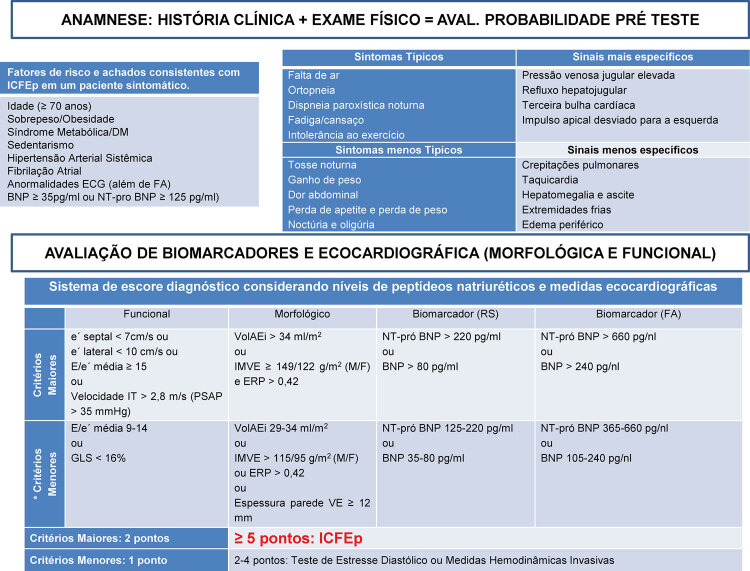
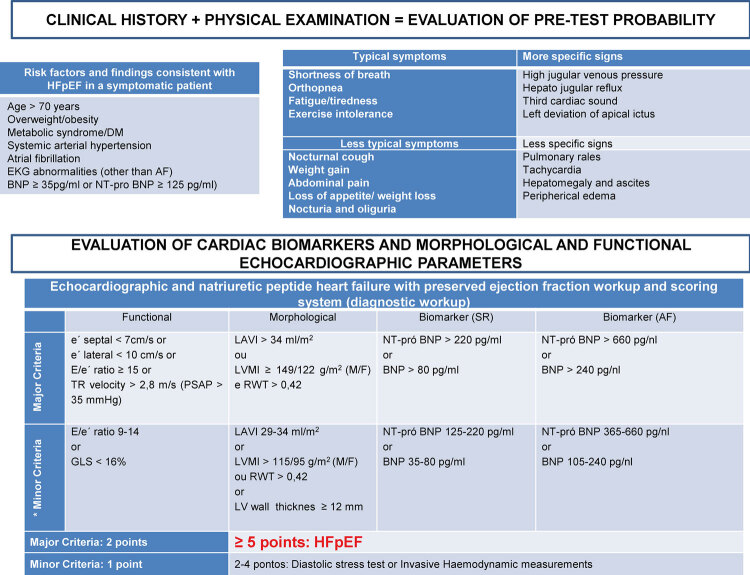
With the increase in the population's life expectancy and the higher frequency of risk factors such as obesity, hypertension and diabetes, an increase in the prevalence of heart failure with preserved ejection fraction (HFpEF) is expected. However, to date, the diagnosis and treatment of patients with HFpEF remain challenging. The syndromic diagnosis of HFpEF includes several etiologies and diseases with specific treatments but has points in common regarding the clinical presentation, laboratory evaluation related to biomarkers, such as BNP and NT-ProBNP, and echocardiographic evaluation of cardiac remodeling and left ventricular diastolic filling pressures. Extensive randomized clinical trials involving the treatment of this condition have failed to demonstrate benefits to the patient, making it necessary to reflect on the diagnosis, mechanisms of morbidity, mortality and reversibility in this syndrome. In this review, the current concepts, controversies and challenges, especially regarding diagnosis, will be addressed, critically analyzing the European Heart Failure Association score for the diagnosis of HFpEF.
Com o aumento da expectativa de vida da população e a maior frequência de fatores de risco como obesidade, hipertensão arterial e diabetes, espera-se um aumento na prevalência de insuficiência cardíaca com fração de ejeção preservada (ICFEp). Entretanto, no momento, o diagnóstico e o tratamento de pacientes com ICFEp permanecem desafiadores. O diagnóstico sindrômico de ICFEp inclui diversas etiologias e doenças com tratamentos específicos, mas que apresentam pontos em comum em relação à apresentação clínica e à avaliação laboratorial no que diz respeito aos biomarcadores como BNP e NT-ProBNP, à avaliação ecocardiográfica do remodelamento cardíaco e às pressões de enchimento diastólico ventricular esquerdo. Extensos ensaios clínicos randomizados envolvendo a terapia nesta síndrome falharam na demonstração de benefícios para o paciente, fazendo-se necessária uma reflexão acerca do diagnóstico, dos mecanismos de morbidade, da taxa de mortalidade e da reversibilidade. Na revisão, serão abordados os conceitos atuais, as controvérsias e, especialmente, os desafios no diagnóstico da ICFEp através de uma análise crítica do escore da European Heart Failure Association.
Conflict of interest statement
Potencial Conflito de Interesse
Declaro não haver conflito de interesses pertinentes.
Figures
References
-
- Pieske B, Tschöpe C, de Boer RA, Fraser AG, Anker SD, Donal E. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC) 10.1093/eurheartj/ehz641Eur Heart J. 2019;40(40):3297–3317. - PubMed
-
- Van Riet EES, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH, et al. Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. 10.1002/ejhf.483Eur J Heart Fail. 2016;18(3):242–252. - PubMed
-
- Seferovic PM, Petrie MC, Filippatos GS, Anker SD, Rosano G, Bauersachs J, et al. Type 2 diabetes mellitus and heart failure: a position statement from the Heart Failure Association of the European Society of Cardiology. 10.1002/ejhf.1170Eur J Heart Fail. 2018;20(5):853–872. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. 10.1002/ejhf.592Eur J Heart Fail. 2016;18(8):891–975. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
