Recent advances in the management of pulmonary hypertension with interstitial lung disease
- PMID: 35831007
- PMCID: PMC9724812
- DOI: 10.1183/16000617.0220-2021
Recent advances in the management of pulmonary hypertension with interstitial lung disease
Abstract
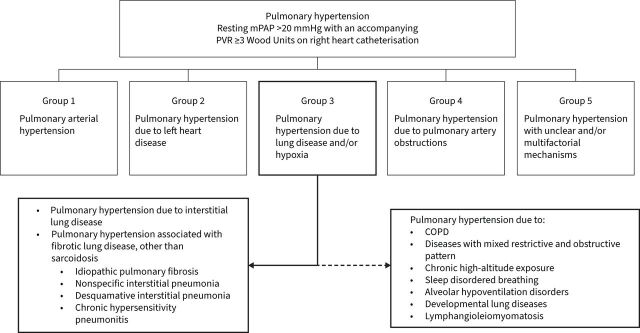
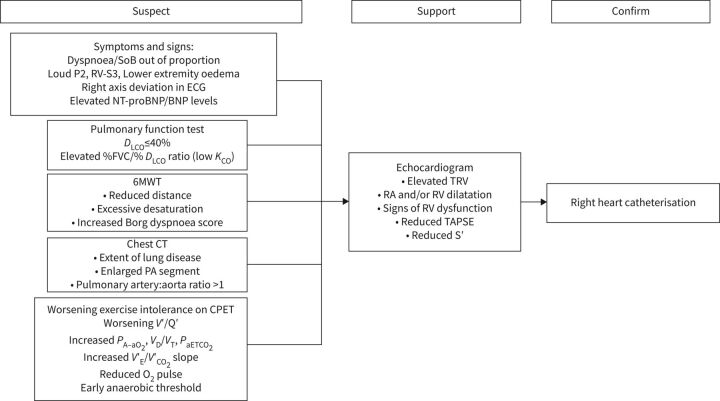
Pulmonary hypertension (PH) is known to complicate various forms of interstitial lung disease (ILD), including idiopathic pulmonary fibrosis, the interstitial pneumonias and chronic hypersensitivity pneumonitis. Pathogenesis of PH-ILD remains incompletely understood, and probably has overlap with other forms of pre-capillary pulmonary hypertension. PH-ILD carries a poor prognosis, and is associated with increased oxygen requirements, and a decline in functional capacity and exercise tolerance. Despite most patients having mild-moderate pulmonary hypertension, more severe pulmonary hypertension and signs of right heart failure are observed in a subset of cases. Clinical suspicion and findings on pulmonary function, computed tomography and echocardiography are often the initial steps towards diagnosis. Definitive diagnosis is obtained by right heart catheterisation demonstrating pre-capillary pulmonary hypertension. Drugs approved for pulmonary arterial hypertension have been investigated in several randomised controlled trials in PH-ILD patients, leading to discouraging results until the recent INCREASE study. This review provides an overview of the current understanding, approach to diagnosis and recent advances in treatment.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: A.B. Waxman reports grants from United Therapeutics, Gossamer and Altavant, and personal fees from ARIA-CV and Acceleron, outside the submitted work. Conflict of interest: D. Elia has nothing to disclose. Conflict of interest: Y. Adir reports personal fees from TEVA, SANOFI, Bayer and Pfizer, and grants and personal fees from GSK, AstraZeneca and Janssen, outside the submitted work; Conflict of interest: M. Humbert reports grants or contracts from Acceleron, Janssen and Merck to his institution; consulting fees from Acceleron, Janssen and Merck (Steering Committees for pulmonary hypertension); payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from AOP, Janssen and Merck; and participation on Advisory Boards for Acceleron, Janssen, Merck and United Therapeutics. Conflict of interest: S. Harari reports personal fees from Roche, grants and personal fees from AstraZeneca and Boehringer Ingelheim, outside the submitted work.
Figures