

The 'prostate-muscle index': a simple pelvic cavity measurement predicting estimated blood loss and console time in robot-assisted radical prostatectomy
- PMID: 35831361
- PMCID: PMC9279306
- DOI: 10.1038/s41598-022-16202-6
The 'prostate-muscle index': a simple pelvic cavity measurement predicting estimated blood loss and console time in robot-assisted radical prostatectomy
Abstract
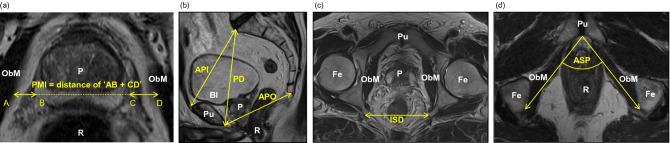
This study was to show the impact of 'prostate-muscle index (PMI)', which we developed as a novel pelvic cavity measurement, in patients undergoing robot-assisted radical prostatectomy (RARP). We defined PMI as the 'distance between the inner edge of the obturator internus muscle and the lateral edge of the prostate at the magnetic resonance imaging (MRI) slice showing the maximum width of the prostate'. Seven hundred sixty patients underwent RARP at the University of Tokyo Hospital from November 2011 to December 2018. MRI results were unavailable in 111 patients. In total, 649 patients were eligible for this study. Median values of blood loss and console time were 300 mL and 168 min. In multivariate analysis, body mass index (BMI), prostate volume-to-pelvic cavity index (PV-to-PCI), PMI, and surgical experience were significantly associated with blood loss > 300 mL (P = 0.0002, 0.002, < 0.0001, and 0.006 respectively). Additionally, BMI, PMI, and surgical experience were also significantly associated with console time > 160 min in multivariate analysis (P = 0.04, 0.004, and < 0.0001, respectively). In conclusion, PMI may provide useful information to surgeons and patients in preoperative decision-making.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Walz J, et al. A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy: An update. Eur. Urol. 2016;70(2):301–311. doi: 10.1016/j.eururo.2016.01.026. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
