

Comment
doi: 10.1038/s41380-022-01688-3.
Epub 2022 Jul 13.
Autoimmune obsessive-compulsive disorder with novel anti-CNS autoantibodies in cerebrospinal fluid
Affiliations
- PMID: 35831487
- PMCID: PMC9718664
- DOI: 10.1038/s41380-022-01688-3
Item in Clipboard
Comment
Autoimmune obsessive-compulsive disorder with novel anti-CNS autoantibodies in cerebrospinal fluid
Mol Psychiatry.
2022 Oct.
No abstract available
Conflict of interest statement
HU: Shareholder of the Veobrain. KD: Steering Committee Neurosciences, Janssen. LTvE: Advisory boards, lectures, or travel grants within the last 3 years: Roche, Eli Lilly, Janssen-Cilag, Novartis, Shire, UCB, GSK, Servier, Janssen and Cyberonics. All other authors declare no potential competing interests.
Figures
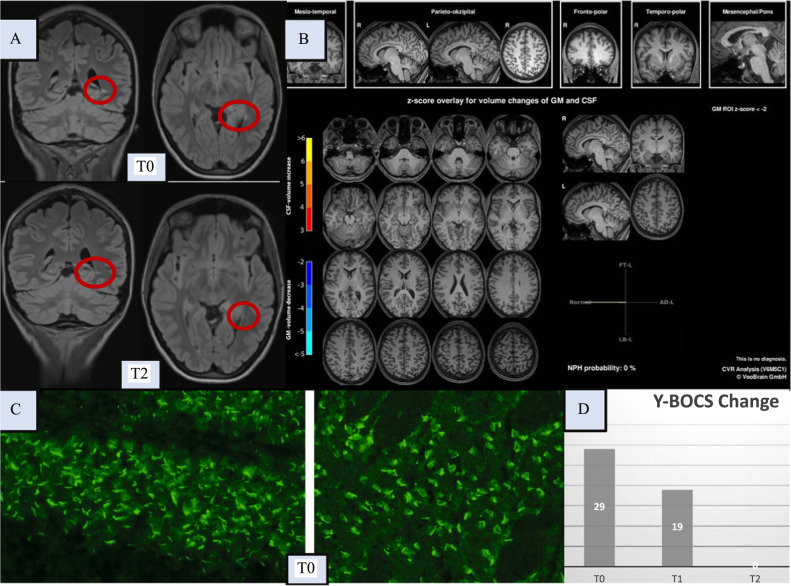
Here, the magnetic resonance imaging (MRI) findings of the brain, the autoantibody findings, and the clinical course based on the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) scores are shown. Brain [18F]fluorodeoxyglucose positron emission tomography (FDG-PET) identified unremarkable findings, and no evidence of malignancy was identified in the whole body FDG-PET. Optical coherence tomography and electroencephalography were normal (these normal findings are not shown). A The left upper row shows the conspicuous FLAIR MRI findings of the brain with a solitary lesion in the left tapetum (at T0), atypical for age in location and localization and potentially (post)inflammatory, but the MRI criteria for multiple sclerosis were not met. In addition, a pineal gland cyst was found loco typico without a space-occupying effect (max. 11 mm in diameter; not shown in detail). The lower images show a regressive lesion in the left tapetum after clinical full remission (at T2, approximately 7 weeks after steroid pulse treatment). B A combined volume- and region-based analysis method (CVR; https://www.veobrain.com/?page=veomorph ) detected no atrophy at T0. At time point T2, there was no relevant change (not shown). C In the cerebrospinal fluid (CSF), autoantibodies against granule cell cilia were found in the hippocampus (left in the bottom row; “rings and rods” pattern) and in neurons of the cortex (right in the bottom row; at T0). In addition, several large vessels were stained (not shown). The tissue-based assay using serum material revealed non-specific findings (not shown). The well-characterized anti-central nervous system autoantibodies against intracellular antigens (Yo/Hu/CV2/CRMP5/Ri/Ma1/2/SOX1/Tr/Zic4/GAD65/amphiphysin) or glial structures (AQP4/MOG) in serum and against cell surface antigens (NMDA-R/LGI1/CASPR2/AMPA1/2-R/GABA-B-R/DPPX) in serum and CSF remained unremarkable (not shown). Additional CSF analyses identified pleocytosis, with a white blood cell count of 10/µl (reference <5/µl); intrathecal immunoglobulin (Ig) synthesis of two isotypes, IgG (53%) and IgA (48%; reference both <10%); an elevated IgG index of 1.37 (reference <0.7); and CSF-specific oligoclonal bands. In contrast, the albumin quotient was normal, and pathogen testing of the CSF remained unremarkable. Elevated specific antibody indices (AIs) for HSV (2.3; reference <1.5) and VZV (2.8; reference <1.5) suggested polyclonal IgG synthesis, but the MRZ reaction remained negative (i.e., AIs for measles and rubella were negative). D The patient showed an initial Y-BOCS score of 29 points (at T0). At T1, immediately after steroid pulse treatment, the patient was able to better distance herself from the obsessive-compulsive symptoms (OCS), and the Y-BOCS score decreased to 19 points. Full remission of OCS (Y-BOCS score: 0) was evident at T2 (approximately 7 weeks after steroid pulse treatment). Neuropsychological testing of attentional performances revealed an improvement in reaction time (alertness with/without warning tone) at the time of the second assessment (directly after stopping steroids; not shown).
Comment on
-
Treatment resistance in psychiatry: state of the art and new directions.Mol Psychiatry. 2022 Jan;27(1):58-72. doi: 10.1038/s41380-021-01200-3. Epub 2021 Jul 13. Mol Psychiatry. 2022. PMID: 34257409 Free PMC article. Review.
References
-
- Endres D, Lüngen E, Hasan A, Kluge M, Fröhlich S, Lewerenz J, et al. Clinical manifestations and immunomodulatory treatment experiences in psychiatric patients with suspected autoimmune encephalitis: a case series of 91 patients from Germany. Mol Psychiatry. 2022. 10.1038/s41380-021-01396-4. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
