

Effect of Comorbidity Burden and Polypharmacy on Poor Functional Outcome in Acute Ischemic Stroke
- PMID: 35831611
- PMCID: PMC10014774
- DOI: 10.1007/s00062-022-01193-8
Effect of Comorbidity Burden and Polypharmacy on Poor Functional Outcome in Acute Ischemic Stroke
Abstract
Purpose: Comorbidities and polypharmacy are risk factors for worse outcome in stroke. However, comorbidities and polypharmacy are mostly studied separately with various approaches to assess them. We aimed to analyze the impact of comorbidity burden and polypharmacy on functional outcome in acute ischemic stroke (AIS) patients undergoing mechanical thrombectomy (MT).
Methods: Acute ischemic stroke patients with large vessel occlusion (LVO) treated with MT from a prospective observational study were analyzed. Relevant comorbidity burden was defined as a Charlson Comorbidity Index (CCI) score ≥ 2, polypharmacy as the intake of ≥ 5 medications at time of stroke onset. Favorable outcome was a score of 0-2 on the modified Rankin scale at 90 days after stroke. The effect of comorbidity burden and polypharmacy on favorable outcome was studied via multivariable regression analysis.
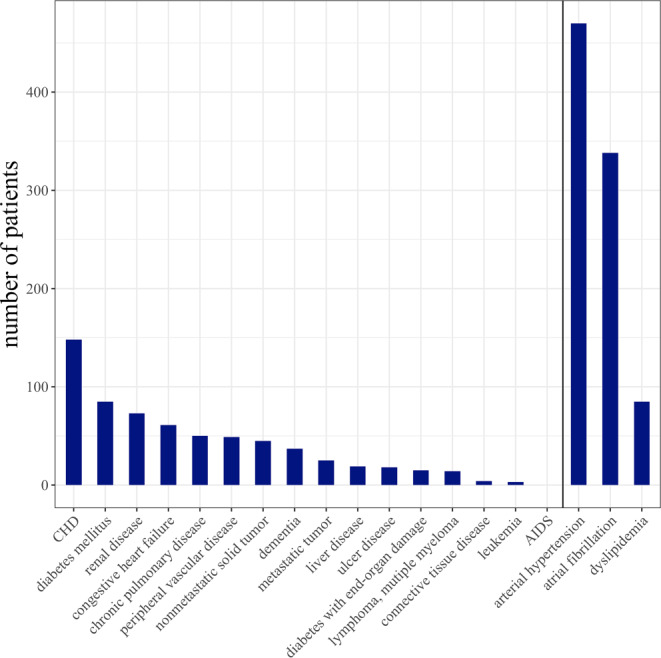
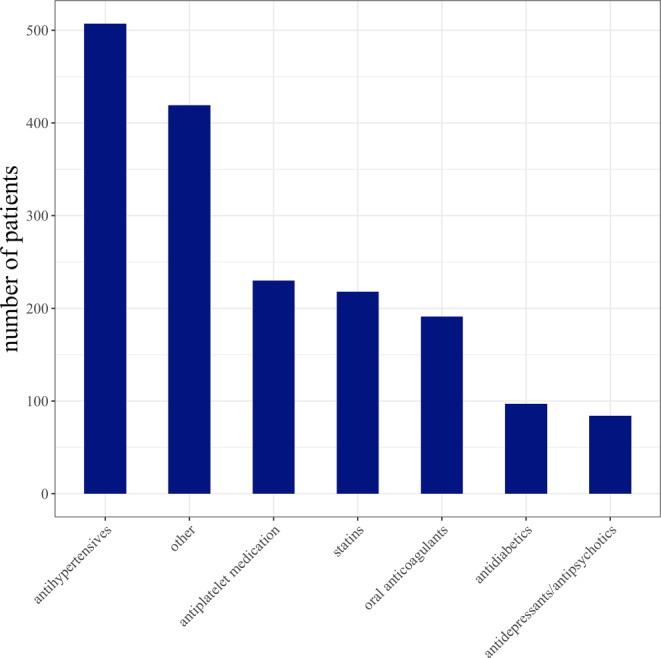
Results: Of 903 patients enrolled, 703 AIS patients (mean age 73.4 years, 54.9% female) with anterior circulation LVO were included. A CCI ≥ 2 was present in 226 (32.1%) patients, polypharmacy in 315 (44.8%) patients. Favorable outcome was less frequently achieved in patients with a CCI ≥ 2 (47, 20.8% vs. 172, 36.1%, p < 0.001), and in patients with polypharmacy (69, 21.9% vs. 150, 38.7%, p < 0.001). In multivariable regression analysis including clinical covariates, a CCI ≥ 2 was associated with lower odds of favorable outcome (odds ratio, OR 0.52, 95% confidence interval, 95% CI 0.33-0.82, p = 0.005), while polypharmacy was not (OR 0.81, 95% CI 0.52-1.27, p = 0.362).
Conclusion: Relevant comorbidity burden and polypharmacy are common in AIS patients with LVO, with comorbidity burden being a risk factor for poor outcome.
Keywords: Acute stroke; Charlson Comorbidity Index; Clinical outome; Large vessel occlusion; Thrombectomy.
© 2022. The Author(s).
Conflict of interest statement
E. Barow, A.-C. Probst, H. Pinnschmidt, M. Heinze, M. Jensen, D.L. Rimmele, F. Flottmann, G. Broocks, J. Fiehler, C. Gerloff and G. Thomalla declare that they have no competing interests.
Figures
Similar articles
-
Comorbidity burden and outcomes after mechanical thrombectomy for large vessel occlusion: A retrospective analysis.J Stroke Cerebrovasc Dis. 2024 Aug;33(8):107778. doi: 10.1016/j.jstrokecerebrovasdis.2024.107778. Epub 2024 May 23. J Stroke Cerebrovasc Dis. 2024. PMID: 38795797
-
Polypharmacy, functional outcome and treatment effect of intravenous alteplase for acute ischaemic stroke.Eur J Neurol. 2021 Feb;28(2):532-539. doi: 10.1111/ene.14566. Epub 2020 Oct 28. Eur J Neurol. 2021. PMID: 33015924 Clinical Trial.
-
An Initial High National Institutes of Health Stroke Scale Score and Any Intracranial Hemorrhage Are Independent Factors for a Poor Outcome in Nonagenarians Treated with Thrombectomy for Acute Large Vessel Occlusion: The Tokyo/Tama-REgistry of Acute Endovascular Thrombectomy (TREAT) Study.World Neurosurg. 2022 Sep;165:e325-e330. doi: 10.1016/j.wneu.2022.06.038. Epub 2022 Jun 16. World Neurosurg. 2022. PMID: 35717017
-
Intravenous thrombolysis prior to mechanical thrombectomy in large vessel occlusions.Ann Neurol. 2019 Sep;86(3):395-406. doi: 10.1002/ana.25544. Epub 2019 Jul 22. Ann Neurol. 2019. PMID: 31282044
-
Mechanical Thrombectomy for Mild Acute Ischemic Stroke with Large-Vessel Occlusion: A Systematic Review and Meta-Analysis.Cerebrovasc Dis. 2022;51(5):615-622. doi: 10.1159/000523838. Epub 2022 Apr 4. Cerebrovasc Dis. 2022. PMID: 35378529
Cited by
-
Impact of prior antiplatelet therapy on safety and efficacy of alteplase in acute ischemic stroke: a systematic review and meta-analysis.Neurol Sci. 2025 Jun;46(6):2461-2478. doi: 10.1007/s10072-025-08024-x. Epub 2025 Feb 22. Neurol Sci. 2025. PMID: 39985653 Free PMC article.
-
Self-reported life-space mobility in the first year after ischemic stroke: longitudinal findings from the MOBITEC-Stroke project.J Neurol. 2023 Aug;270(8):3992-4003. doi: 10.1007/s00415-023-11748-5. Epub 2023 May 4. J Neurol. 2023. PMID: 37140729 Free PMC article.
-
Designing machine learning for big data: A study to identify factors that increase the risk of ischemic stroke and prognosis in hypertensive patients.Digit Health. 2024 Oct 8;10:20552076241288833. doi: 10.1177/20552076241288833. eCollection 2024 Jan-Dec. Digit Health. 2024. PMID: 39386108 Free PMC article.
-
The impact of comorbidity burden on outcomes following endovascular thrombectomy for acute ischemic stroke: A nationwide prospective observational study.Eur Stroke J. 2025 Apr 12:23969873251332136. doi: 10.1177/23969873251332136. Online ahead of print. Eur Stroke J. 2025. PMID: 40219850 Free PMC article.
References
-
- Asplund K, Karvanen J, Giampaoli S, Jousilahti P, Niemela M, Broda G, Cesana G, Dallongeville J, Ducimetriere P, Evans A, Ferrieres J, Haas B, Jorgensen T, Tamosiunas A, Vanuzzo D, Wiklund PG, Yarnell J, Kuulasmaa K, Kulathinal S, Project M. Relative risks for stroke by age, sex, and population based on follow-up of 18 European populations in the MORGAM project. Stroke. 2009;40:2319–2326. doi: 10.1161/STROKEAHA.109.547869. - DOI - PubMed
-
- Gallacher KI, Batty GD, McLean G, Mercer SW, Guthrie B, May CR, Langhorne P, Mair FS. Stroke, multimorbidity and polypharmacy in a nationally representative sample of 1,424,378 patients in Scotland: implications for treatment burden. BMC Med. 2014;12:151. doi: 10.1186/s12916-014-0151-0. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
