

Pharmacist-led medication reconciliation at patient discharge: a tool to reduce healthcare utilization? an observational study in patients 65 years or older
- PMID: 35831783
- PMCID: PMC9281036
- DOI: 10.1186/s12877-022-03192-3
Pharmacist-led medication reconciliation at patient discharge: a tool to reduce healthcare utilization? an observational study in patients 65 years or older
Abstract
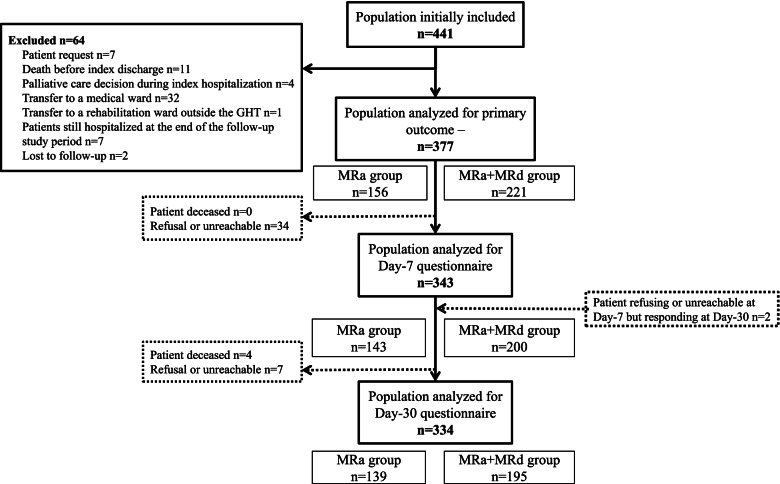
Background: Older patients often experience adverse drug events (ADEs) after discharge that may lead to unplanned readmission. Medication Reconciliation (MR) reduces medication errors that lead to ADEs, but results on healthcare utilization are still controversial. This study aimed to assess the effect of MR at discharge (MRd) provided to patients aged over 65 on their unplanned rehospitalization within 30 days and on both patients' experience of discharge and their knowledge of their medication.
Methods: An observational multicenter prospective study was conducted in 5 hospitals in Brittany, France.
Results: Patients who received both MR on admission (MRa) and MRd did not have significantly fewer deaths, unplanned rehospitalizations and/or emergency visits related to ADEs (OR = 1.6 [0.7 to 3.6]) or whatever the cause (p = 0.960) 30 days after discharge than patients receiving MRa alone. However, patients receiving both MRa and MRd were more likely to feel that their discharge from the hospital was well organized (p = 0.003) and reported more frequently that their community pharmacist received information about their hospital stay (p = 0.036).
Conclusions: This study found no effect of MRd on healthcare utilization 30 days after discharge in patients over 65, but the process improved patients' experiences of care continuity. Further studies are needed to better understand this positive impact on their drug care pathway in order to improve patients' ownership of their drugs, which is still insufficient. Improving both the interview step between pharmacist and patient before discharge and the transmission of information from the hospital to primary care professionals is needed to enhance MR effectiveness.
Trial registration: NCT04018781 July 15, 2019.
Keywords: Adverse Drug Event; Discharge; Experience; Medication Reconciliation; Older people.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Schwab C, Korb-Savoldelli V, Escudie JB, Fernandez C, Durieux P, Saint-Jean O, et al. Iatrogenic risk factors associated with hospital readmission of elderly patients: A matched case-control study using a clinical data warehouse. J Clin Pharm Ther. 2018;43(3):393–400. doi: 10.1111/jcpt.12670. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
