

Description of a New Labyrinthine Dehiscence: Horizontal Semicircular Canal Dehiscence at the Tympanic Segment of the Facial Nerve
- PMID: 35832172
- PMCID: PMC9271764
- DOI: 10.3389/fneur.2022.879149
Description of a New Labyrinthine Dehiscence: Horizontal Semicircular Canal Dehiscence at the Tympanic Segment of the Facial Nerve
Abstract
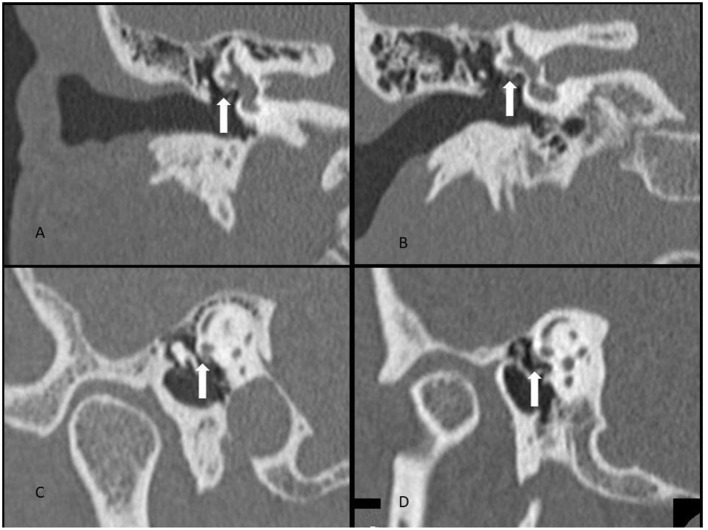
Objective: This report is a case series of patients with findings suspicious for a labyrinthine dehiscence syndrome not previously described in the medical literature. We describe the clinical and test findings in 16 patients with CT findings suspicious for dehiscence of the ampullated end of the horizontal semicircular canal at the tympanic segment of the facial nerve.
Study design: Observational case series.
Setting: Neurotology vestibular referral center.
Patients: To be included in this study the patients were seen at our center in 2019 and had a high-resolution CT scan with a collimation of 0.6 mm. Patients who were identified as having findings suspicious for dehiscence of bone where the facial nerve crosses the ampullated end of the horizontal semicircular canal (HSC-FND) were identified and further analyzed.
Interventions: Case series retrospective record review of patient symptoms, physical findings, audiometry, vestibular testing, and CT scans was performed. CT findings of other dehiscent sites were noted. A comparison to surgically treated perilymph fistula (PLF) patients of the same period was performed.
Main outcome measures: History and physical exam were reviewed for auditory symptoms, vestibular symptoms, and exacerbating factors. and. Audiometry and vestibular testing were reviewed to determine which tests were most likely to be abnormal. CT scans were independently graded according to degree of suspicion for HSC-FND. Finally, patients with HSC-FND as the sole dehiscence identified were compared to those who had HSC-FND plus other dehiscent sites (HSC-FND+O) and to the group of surgically treated PLF patients.
Results: Of 18 patients, 16 met inclusion criteria. Nine (56%) of those suspicious for HSC-FND had dehiscences in other parts of the labyrinth. Additional dehiscent sites included: six superior semicircular canal dehiscences (SSCD), two cochlear facial dehiscences and one cochlear carotid dehiscence. The most common auditory symptoms were autophony followed by tinnitus and aural fullness. The most common vestibular symptoms were pulsion sensation (feeling of being pushed to one side) followed by vertigo spells. The most common exacerbating factors for vertigo were straining, and sound. The most commonly abnormal vestibular test was nasal Valsalva testing, which was positive in all but one patient. Anamnesis and examination observations were similar in both groups, but the HSC-FND group were less likely to demonstrate a caloric weakness or an abnormal ECOG compared to the HSC-FND+O group. Of note, cVEMP was more often found to have lower thresholds in the HSC-FND group compared to the HSC-FND+O group. An example case is highlighted. Comparison to the PLF patients revealed statistically significant difference in the presenting symptoms of autophony, fullness and pulsion sensation. When comparing testing, HSC-FND patients were more likely to have an abnormal cVEMP and PLF patients were more likely to have asymmetric hearing. The incidence of bilateral disease was also more common among the HSC-FND patients than the PLF patients.
Conclusions: A new labyrinthine dehiscence has been described to occur where the tympanic segment of the facial nerve crosses over the ampullated end of the horizontal semicircular canal. HSC-FND patients can present in a similar manner as HSC-FND+O patients with similar test findings except as mentioned above. The identification of one dehiscence such as SSCD does not preclude the presence of another dehiscence such as HSC-FND. HSC-FND could be the source of persistent symptoms post SSCD surgery as illustrated in the case presented. HSC-FND patients seem to identify themselves compared to PLF patients by a much more likely presenting symptoms of autophony, fullness, pulsion, abnormal cVEMP, bilaterality of disease, and symmetric hearing.
Keywords: Tullio phenomenon; dehiscence; facial nerve; horizontal semicircular canal; perilymphatic fistula; third mobile window; vertigo.
Copyright © 2022 Gianoli, Soileau and Shore.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Posterior semicircular canal dehiscence: CT prevalence and clinical symptoms.Otol Neurotol. 2014 Feb;35(2):310-4. doi: 10.1097/MAO.0000000000000183. Otol Neurotol. 2014. PMID: 24366470
-
Superior semicircular canal dehiscence presenting as postpartum vertigo.Otol Neurotol. 2006 Sep;27(6):756-68. doi: 10.1097/01.mao.0000227894.27291.9f. Otol Neurotol. 2006. PMID: 16936563 Review.
-
Variety of audiologic manifestations in patients with superior semicircular canal dehiscence.Otol Neurotol. 2010 Jan;31(1):2-10. doi: 10.1097/mao.0b013e3181bc35ce. Otol Neurotol. 2010. PMID: 20050265
-
Prevalence of Cochlear-Facial and Other Non-Superior Semicircular Canal Third Window Dehiscence on High-Resolution Temporal Bone CT.AJNR Am J Neuroradiol. 2023 Nov;44(11):1309-1313. doi: 10.3174/ajnr.A8032. Epub 2023 Oct 26. AJNR Am J Neuroradiol. 2023. PMID: 37884302 Free PMC article.
-
Characteristics and management of superior semicircular canal dehiscence.J Neurol Surg B Skull Base. 2012 Dec;73(6):365-70. doi: 10.1055/s-0032-1324397. Epub 2012 Aug 8. J Neurol Surg B Skull Base. 2012. PMID: 24294552 Free PMC article. Review.
Cited by
-
Characteristics of the Facial Canal-Lateral Canal Dehiscence: The Under-recognized Third Window.OTO Open. 2025 Feb 17;9(1):e70085. doi: 10.1002/oto2.70085. eCollection 2025 Jan-Mar. OTO Open. 2025. PMID: 39963505 Free PMC article.
-
Why should multiple dehiscences of the otic capsule be considered before surgically treating patients with superior semicircular canal dehiscence? A radiological monocentric review and a case series.Front Neurol. 2023 Aug 8;14:1209567. doi: 10.3389/fneur.2023.1209567. eCollection 2023. Front Neurol. 2023. PMID: 37614976 Free PMC article. Review.
-
Posterior Semicircular Canal Dehiscence with Vestibulo-Ocular Reflex Reduction for the Affected Canal at the Video-Head Impulse Test: Considerations to Pathomechanisms.Audiol Res. 2024 Mar 24;14(2):317-332. doi: 10.3390/audiolres14020028. Audiol Res. 2024. PMID: 38666899 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous