

The ABC-Stroke Score Refines Stroke Risk Stratification in Patients With Atrial Fibrillation at the Emergency Department
- PMID: 35833107
- PMCID: PMC9271836
- DOI: 10.3389/fmed.2022.830580
The ABC-Stroke Score Refines Stroke Risk Stratification in Patients With Atrial Fibrillation at the Emergency Department
Abstract
Aims: To evaluate the performance of the ABC (Age, Biomarkers, Clinical history) and CHA2DS2-VASc stroke scores under real-world conditions in an emergency setting.
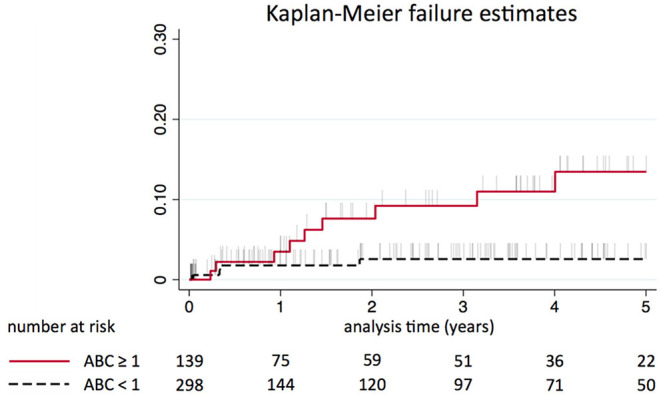
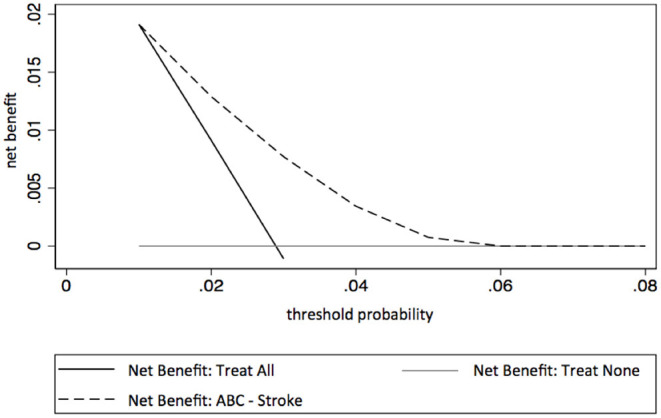
Methods and results: The performance of the biomarker-based ABC-stroke score and the clinical variable-based CHA2DS2-VASc score for stroke risk assessment were prospectively evaluated in a consecutive series of 2,108 patients with acute symptomatic atrial fibrillation at a tertiary care emergency department. Performance was assessed according to methods for the development and validation of clinical prediction models by Steyerberg et al. and the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis. During a cumulative observation period of 3,686 person-years, the stroke incidence rate was 1.66 per 100 person-years. Overall, the ABC-stroke and CHA2DS2-VASc scores revealed respective c-indices of 0.64 and 0.55 for stroke prediction. Risk-class hazard ratios comparing moderate to low and high to low were 3.51 and 2.56 for the ABC-stroke score and 1.10 and 1.62 for the CHA2DS2-VASc score. The ABC-stroke score also provided improved risk stratification in patients with moderate stroke risk according to the CHA2DS2-VASc score, who lack clear recommendations regarding anticoagulation therapy (HR: 4.35, P = 0.001). Decision curve analysis indicated a superior net clinical benefit of using the ABC-stroke score.
Conclusion: In a large, real-world cohort of patients with acute atrial fibrillation in the emergency department, the ABC-stroke score was superior to the guideline-recommended CHA2DS2-VASc score at predicting stroke risk and refined risk stratification of patients labeled moderate risk by the CHA2DS2-VASc score, potentially easing treatment decision-making.
Keywords: biomarkers; performance evaluation; prediction score; stroke; symptomatic atrial fibrillation; validation.
Copyright © 2022 Niederdöckl, Oppenauer, Schnaubelt, Cacioppo, Buchtele, Warenits, Laggner, Schütz, Bögl, Ruzicka, Gupta, Lutnik, Sheikh Rezaei, Wolzt, Herkner, Domanovits, Laggner, Schwameis and Hijazi.
Conflict of interest statement
ZH reports personal fees from Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer and Roche Diagnostics for lectures, personal fees from Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Roche Diagnostics for consulting, and grants from the Swedish Society for Medical Research (S17-0133) and the Swedish Heart-Lung Foundation (20170718), outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Validation of a Modified CHA2DS2-VASc Score for Stroke Risk Stratification in Asian Patients With Atrial Fibrillation: A Nationwide Cohort Study.Stroke. 2016 Oct;47(10):2462-9. doi: 10.1161/STROKEAHA.116.013880. Epub 2016 Sep 13. Stroke. 2016. PMID: 27625386
-
Performance of the ABC Scores for Assessing the Risk of Stroke or Systemic Embolism and Bleeding in Patients With Atrial Fibrillation in ENGAGE AF-TIMI 48.Circulation. 2019 Feb 5;139(6):760-771. doi: 10.1161/CIRCULATIONAHA.118.038312. Circulation. 2019. PMID: 30586727 Free PMC article. Clinical Trial.
-
Incidence and prediction of ischemic stroke among atrial fibrillation patients with end-stage renal disease requiring dialysis.Heart Rhythm. 2014 Oct;11(10):1752-9. doi: 10.1016/j.hrthm.2014.06.021. Epub 2014 Jun 18. Heart Rhythm. 2014. PMID: 24952148
-
Stroke Risk in Atrial Fibrillation: Beyond the CHA2DS2-VASc Score.Curr Cardiol Rep. 2019 Jul 27;21(9):95. doi: 10.1007/s11886-019-1189-6. Curr Cardiol Rep. 2019. PMID: 31352536 Review.
-
Meta-analysis of CHADS2 versus CHA2DS2-VASc for predicting stroke and thromboembolism in atrial fibrillation patients independent of anticoagulation.Tex Heart Inst J. 2015 Feb 1;42(1):6-15. doi: 10.14503/THIJ-14-4353. eCollection 2015 Feb. Tex Heart Inst J. 2015. PMID: 25873792 Free PMC article. Review.
Cited by
-
Refining Stroke Risk Assessment in Patients with Device-Detected Atrial Fibrillation.J Clin Med. 2024 Dec 27;14(1):82. doi: 10.3390/jcm14010082. J Clin Med. 2024. PMID: 39797165 Free PMC article.
-
The ABC-Stroke Risk Score and Effects of Atrial Fibrillation Screening on Stroke Prevention: Results From the Randomized LOOP Study.J Am Heart Assoc. 2024 Feb 20;13(4):e032744. doi: 10.1161/JAHA.123.032744. Epub 2024 Feb 14. J Am Heart Assoc. 2024. PMID: 38353260 Free PMC article. Clinical Trial.
References
-
- GBD 2015 . Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1659–724. 10.1016/S0140-6736(16)31679-8 - DOI - PMC - PubMed
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. . 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42:373–498. 10.1093/eurheartj/ehaa612 - DOI - PubMed
LinkOut - more resources
Full Text Sources