

Current Advances in PD-1/PD-L1 Blockade in Recurrent Epithelial Ovarian Cancer
- PMID: 35833132
- PMCID: PMC9271774
- DOI: 10.3389/fimmu.2022.901772
Current Advances in PD-1/PD-L1 Blockade in Recurrent Epithelial Ovarian Cancer
Abstract
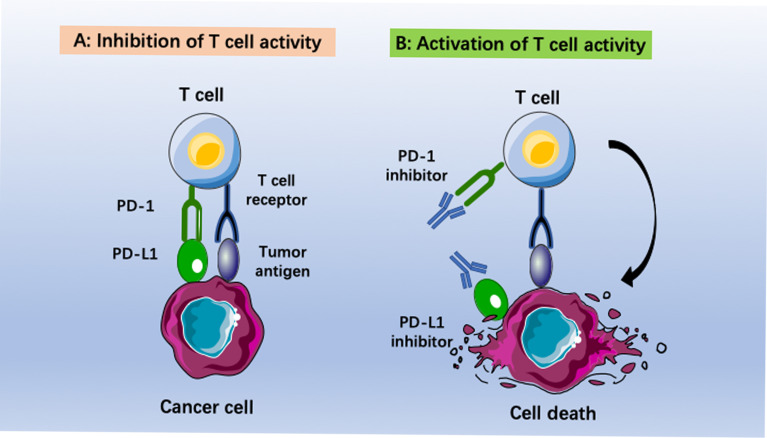
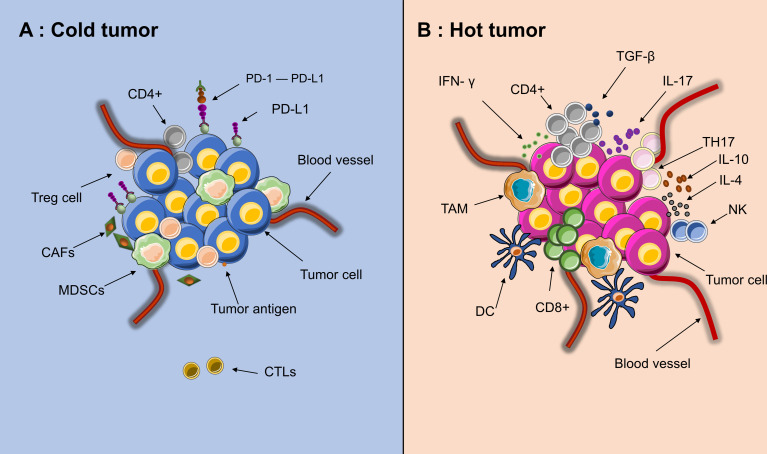
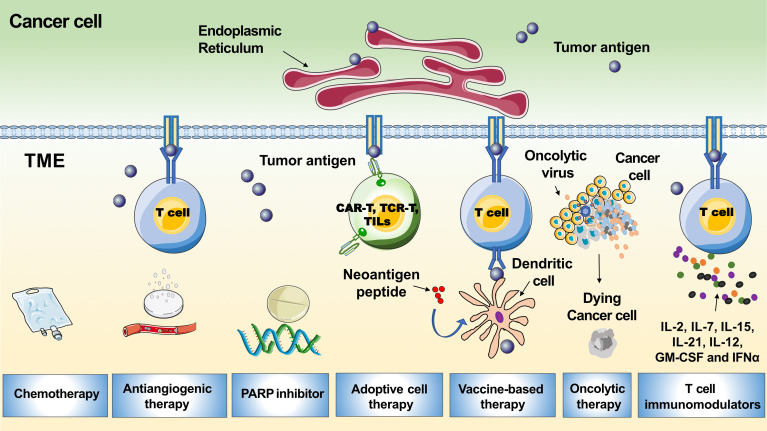
Immunotherapies have revolutionized the treatment of a variety of cancers. Epithelial ovarian cancer is the most lethal gynecologic malignancy, and the rate of advanced tumor progression or recurrence is as high as 80%. Current salvage strategies for patients with recurrent ovarian cancer are rarely curative. Recurrent ovarian cancer is a "cold tumor", predominantly due to a lack of tumor antigens and an immunosuppressive tumor microenvironment. In trials testing programmed death-1 (PD-1)/programmed death ligand 1 (PD-L1) blockade as a monotherapy, the response rate was only 8.0-22.2%. In this review, we illustrate the status of cold tumors in ovarian cancer and summarize the existing clinical trials investigating PD-1/PD-L1 blockade in recurrent ovarian cancer. Increasing numbers of immunotherapy combination trials have been set up to improve the response rate of EOC. The current preclinical and clinical development of immunotherapy combination therapy to convert an immune cold tumor into a hot tumor and their underlying mechanisms are also reviewed. The combination of anti-PD-1/PD-L1 with other immunomodulatory drugs or therapies, such as chemotherapy, antiangiogenic therapies, poly (ADP-ribose) polymerase inhibitors, adoptive cell therapy, and oncolytic therapy, could be beneficial. Further efforts are merited to transfer these results to a broader clinical application.
Keywords: cold tumor; immunotherapy; programmed death ligand 1 (PD-L1); programmed death-1 (PD-1); recurrent ovarian cancer.
Copyright © 2022 Zhang, Cui, Xu, Liu, Yao and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Tumor-associated macrophages and the tumor immune microenvironment of primary and recurrent epithelial ovarian cancer.Hum Pathol. 2018 Apr;74:135-147. doi: 10.1016/j.humpath.2017.12.010. Epub 2017 Dec 27. Hum Pathol. 2018. PMID: 29288043
-
Strategies to synergize PD-1/PD-L1 targeted cancer immunotherapies to enhance antitumor responses in ovarian cancer.Biochem Pharmacol. 2023 Sep;215:115724. doi: 10.1016/j.bcp.2023.115724. Epub 2023 Jul 29. Biochem Pharmacol. 2023. PMID: 37524205 Review.
-
Therapeutic implications of the tumor microenvironment in ovarian cancer patients receiving PD-1/PD-L1 therapy.Front Immunol. 2022 Oct 20;13:1036298. doi: 10.3389/fimmu.2022.1036298. eCollection 2022. Front Immunol. 2022. PMID: 36341388 Free PMC article. Review.
-
Stratification of ovarian tumor pathology by expression of programmed cell death-1 (PD-1) and PD-ligand- 1 (PD-L1) in ovarian cancer.J Ovarian Res. 2018 May 30;11(1):43. doi: 10.1186/s13048-018-0414-z. J Ovarian Res. 2018. PMID: 29843813 Free PMC article.
-
PD-1/PD-L1 Blockade Therapy in Advanced Non-Small-Cell Lung Cancer: Current Status and Future Directions.Oncologist. 2019 Feb;24(Suppl 1):S31-S41. doi: 10.1634/theoncologist.2019-IO-S1-s05. Oncologist. 2019. PMID: 30819829 Free PMC article. Review.
Cited by
-
Immune checkpoint inhibitors in ovarian cancer: where do we go from here?Cancer Drug Resist. 2023 Jun 14;6(2):358-377. doi: 10.20517/cdr.2023.13. eCollection 2023. Cancer Drug Resist. 2023. PMID: 37457131 Free PMC article. Review.
-
Current Understanding on Why Ovarian Cancer Is Resistant to Immune Checkpoint Inhibitors.Int J Mol Sci. 2023 Jun 29;24(13):10859. doi: 10.3390/ijms241310859. Int J Mol Sci. 2023. PMID: 37446039 Free PMC article. Review.
-
A tumor targeted nano micelle carrying astragaloside IV for combination treatment of bladder cancer.Sci Rep. 2024 Jul 31;14(1):17704. doi: 10.1038/s41598-024-66010-3. Sci Rep. 2024. PMID: 39085255 Free PMC article.
-
Treating ICB-resistant cancer by inhibiting PD-L1 via DHHC3 degradation induced by cell penetrating peptide-induced chimera conjugates.Cell Death Dis. 2024 Sep 30;15(9):701. doi: 10.1038/s41419-024-07073-y. Cell Death Dis. 2024. PMID: 39349454 Free PMC article.
-
Platinum-based chemotherapy promotes antigen presenting potential in monocytes of patients with high-grade serous ovarian carcinoma.Front Immunol. 2024 Sep 9;15:1414716. doi: 10.3389/fimmu.2024.1414716. eCollection 2024. Front Immunol. 2024. PMID: 39315092 Free PMC article.
References
-
- Arora T, Mullangi S, Lekkala MR. Ovarian Cancer. In: Statpearls. Treasure Island (FL: StatPearls Publishing LLC; (2021).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials