

Neuromodulation in Chronic Pelvic Pain: A Narrative Review
- PMID: 35834103
- PMCID: PMC9314476
- DOI: 10.1007/s40122-022-00405-w
Neuromodulation in Chronic Pelvic Pain: A Narrative Review
Abstract
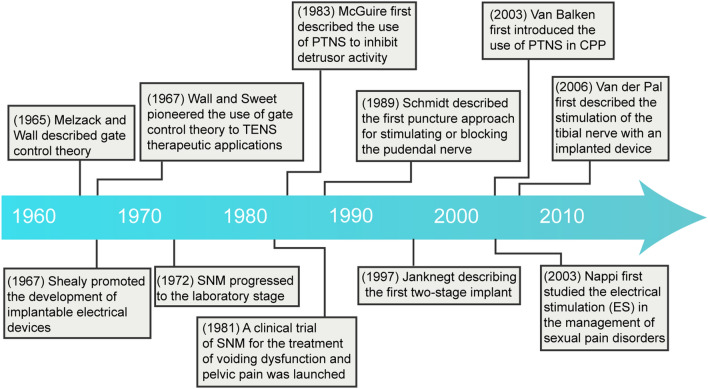
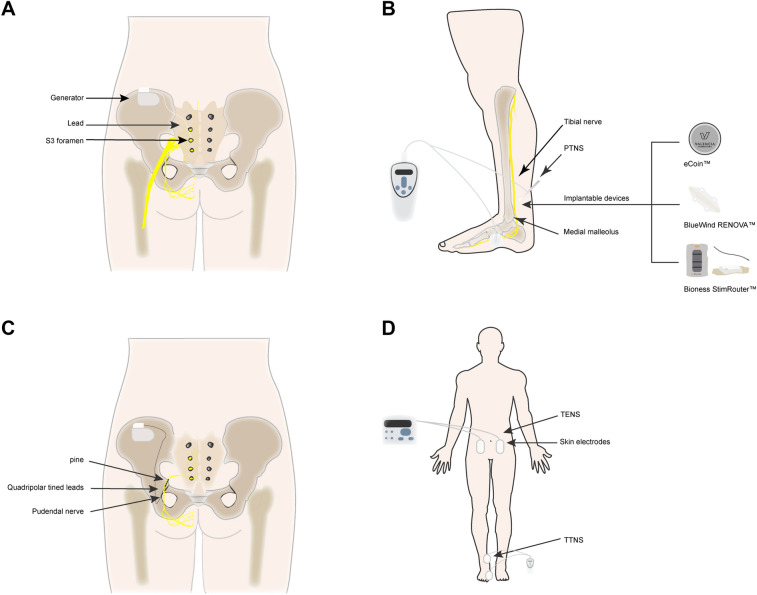
Chronic primary pelvic pain syndrome (CPPPS) is a heterogeneous disease with unknown pathogenesis and a lack of distinct pathological features, which complicates diagnosis and therapy and has a significant impact on patients' daily life. Because pharmacological management is ineffective and long-term use may result in additional system damage, developing a more effective treatment is critical. Neuromodulation has advanced rapidly over the last few decades, and various types of neuromodulations have demonstrated efficacy in the treatment of CPPPS. In this article we discuss the evolution of neuromodulation technology in the treatment of chronic pelvic pain, its application to various subtypes of chronic pelvic pain, and the comparison of relevant efficacy and parameter differences, as well as assess the relative advantages and disadvantages of sacral neuromodulation, percutaneous tibial nerve stimulation , transcutaneous electrical nerve stimulation, electroacupuncture, and pudendal neuromodulation. Furthermore, it was noted that chronic pelvic pain should be evaluated in terms of pain, associated symptoms, psychological problems, and quality of life. Although neuromodulation approaches have been shown to be effective in treating chronic pelvic pain, more extensive multicenter trials are required to confirm this.
Keywords: Chronic pelvic pain; Chronic primary pelvic pain syndrome; Neuromodulation; Percutaneous tibial nerve stimulation; Sacral nerve modulation; Transcutaneous electrical nerve stimulation.
© 2022. The Author(s).
Figures
Similar articles
-
Benefits and Harms of Electrical Neuromodulation for Chronic Pelvic Pain: A Systematic Review.Eur Urol Focus. 2020 May 15;6(3):559-571. doi: 10.1016/j.euf.2019.09.011. Epub 2019 Oct 19. Eur Urol Focus. 2020. PMID: 31636030
-
The Role of Neuromodulation in Chronic Pelvic Pain: A Review Article.Pain Physician. 2022 Jul;25(4):E531-E542. Pain Physician. 2022. PMID: 35793177 Review.
-
Neuromodulation for Management of Chronic Pelvic Pain: A Comprehensive Review.Pain Ther. 2022 Dec;11(4):1137-1177. doi: 10.1007/s40122-022-00430-9. Epub 2022 Sep 15. Pain Ther. 2022. PMID: 36109459 Free PMC article. Review.
-
Neuromodulation for Chronic Pelvic Pain.Curr Urol Rep. 2018 Mar 26;19(5):32. doi: 10.1007/s11934-018-0783-2. Curr Urol Rep. 2018. PMID: 29582185 Review.
-
Neuromodulation in urology, state of the art.Urologia. 2019 Nov;86(4):177-182. doi: 10.1177/0391560319866075. Epub 2019 Aug 1. Urologia. 2019. PMID: 31368415 Review.
Cited by
-
Chronic Overlapping Pain Conditions and Nociplastic Pain.medRxiv [Preprint]. 2024 May 8:2023.06.27.23291959. doi: 10.1101/2023.06.27.23291959. medRxiv. 2024. Update in: HGG Adv. 2025 Jan 09;6(1):100381. doi: 10.1016/j.xhgg.2024.100381. PMID: 38766033 Free PMC article. Updated. Preprint.
-
The Role of Percutaneous Tibial Nerve Stimulation (PTNS) in Low Anterior Resection Syndrome (LARS): A Systematic Review and Meta-analysis.J Gastrointest Cancer. 2023 Dec;54(4):1128-1139. doi: 10.1007/s12029-023-00910-x. Epub 2023 Jan 27. J Gastrointest Cancer. 2023. PMID: 36703030
-
Light-Controlled Electric Stimulation with Organic Electrolytic Photocapacitors Achieves Complex Neuronal Network Activation: Semi-Chronic Study in Cortical Cell Culture and Rat Model.Adv Healthc Mater. 2024 Nov;13(29):e2401303. doi: 10.1002/adhm.202401303. Epub 2024 Aug 13. Adv Healthc Mater. 2024. PMID: 39139004 Free PMC article.
-
Updates in pelvic neuromodulation: the role of pelvic neuromodulation in pelvic disorders.Front Urol. 2024 Mar 15;4:1329305. doi: 10.3389/fruro.2024.1329305. eCollection 2024. Front Urol. 2024. PMID: 40777094 Free PMC article. Review.
-
Chronic overlapping pain conditions and nociplastic pain.HGG Adv. 2025 Jan 9;6(1):100381. doi: 10.1016/j.xhgg.2024.100381. Epub 2024 Nov 4. HGG Adv. 2025. PMID: 39497418 Free PMC article.
References
-
- Engeler D, Baranowski AP, Berghmans B, et al. EAU guidelines on chronic pelvic pain. Arnhem, EAU Guidelines Office; 2022. http://uroweb.org/guidelines/compilations-of-all-guidelines/.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
