

Appropriateness of indirect markers of muscle damage following lower limbs eccentric-biased exercises: A systematic review with meta-analysis
- PMID: 35834532
- PMCID: PMC9282447
- DOI: 10.1371/journal.pone.0271233
Appropriateness of indirect markers of muscle damage following lower limbs eccentric-biased exercises: A systematic review with meta-analysis
Abstract
Purpose: The aim of this review was to (1) characterize the time-course of markers of exercise-induced muscle damage (EIMD) based on the level of maximal voluntary contraction torque loss at 24-48h post-exercise (MVCloss24-48h), (2) identify factors (e.g., exercise and population characteristics) affecting the level of MVCloss24-48h, and (3) evaluate the appropriateness of EIMD markers as indicators of MVCloss24-48h.
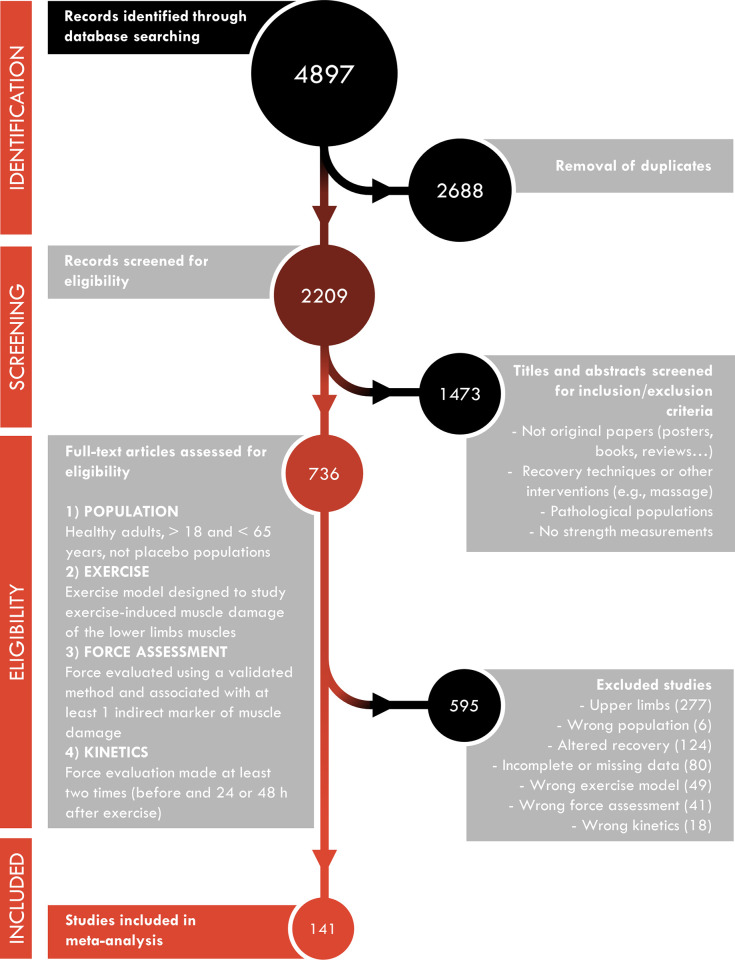
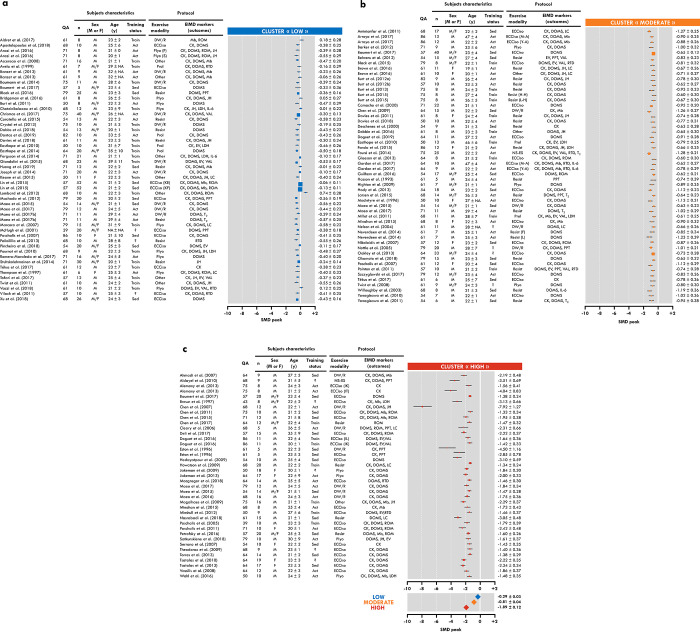
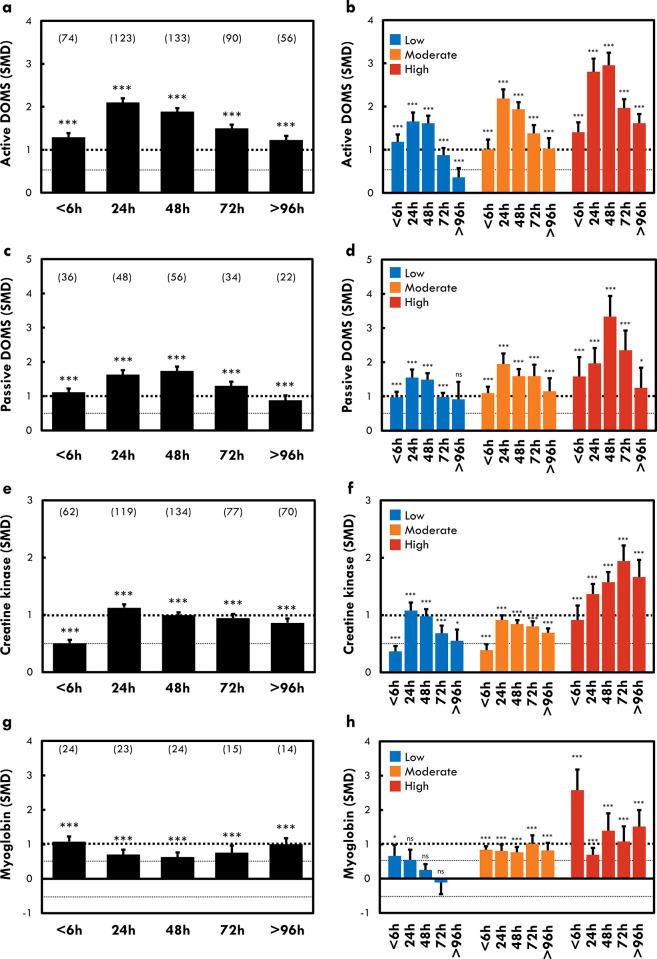
Methods: Magnitude of change of each EIMD markers was normalized using the standardized mean differences method to compare the results from different studies. Time-course of EIMD markers were characterized according to three levels of MVCloss24-48h based on a clustering analysis of the 141 studies included. Association between MVCloss24-48h levels and participant´s characteristics or exercise type/modalities were assessed. Meta-regressions were performed to investigate the associations between MVCloss24-48h and EIMD markers changes at <6h, 24h, 48h, 72h and >96h after exercise.
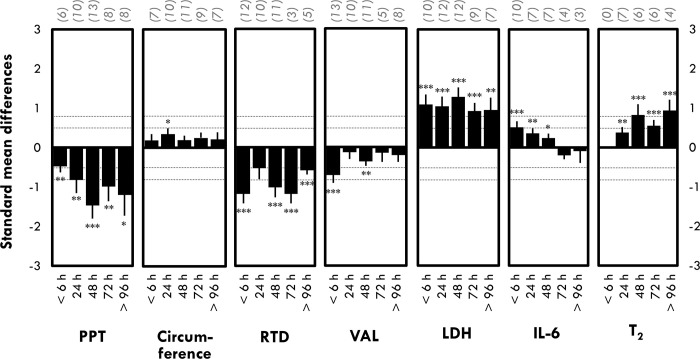
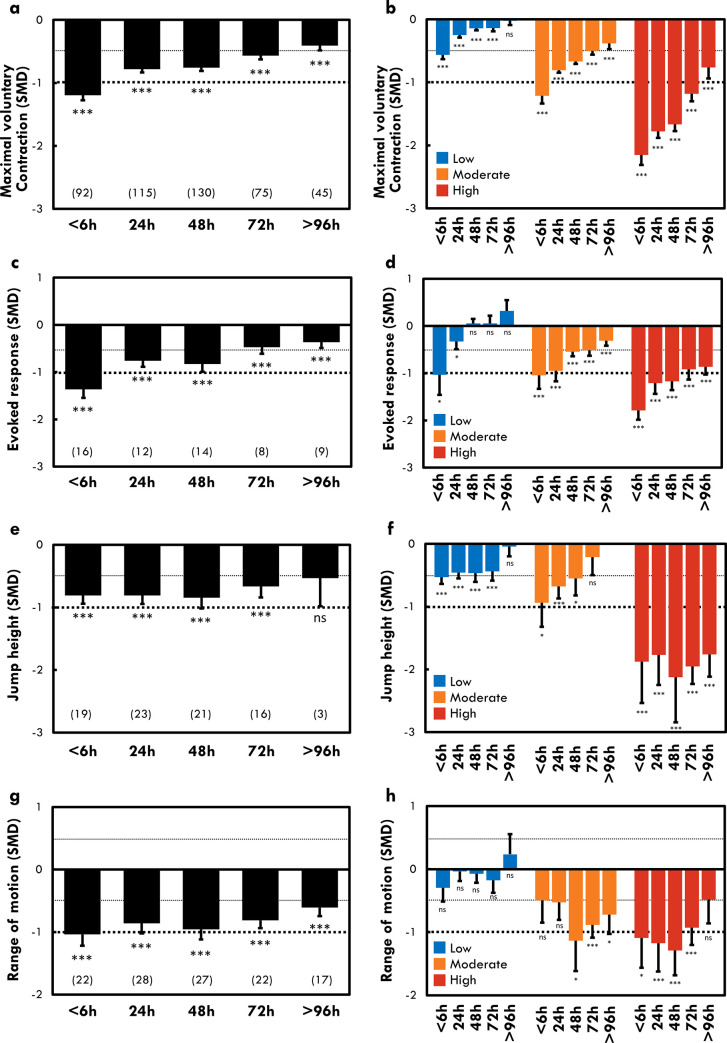
Results: Time-course of EIMD markers recovery differs between levels of MVCloss24-48h. Training status and exercise type/modality were associated with MVCloss24-48h level (p<0.05). MVCloss24-48h was correlated to changes in myoglobin concentration (<6h), jump height (24h) and range of motion (48h) (p<0.001).
Conclusion: As the exercise could differently affect markers as function of the EIMD severity (i.e., MVCloss24-48h levels), different markers should be used as function of the timing of measurement. Mb concentration should be used during the first hours after the exercise (<6h), whereas jump height (24h) and range of motion (48h) could be used as surrogate for maximal voluntary contraction later. Moreover, training status and exercise type/modality could influence the magnitude of MVCloss24-48h.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Ortega-Castillo M, Medina-Porqueres I. Effectiveness of the eccentric exercise therapy in physically active adults with symptomatic shoulder impingement or lateral epicondylar tendinopathy: A systematic review. Journal of science and medicine in sport. 2016;19(6):438–53. Epub 2015/08/26. doi: 10.1016/j.jsams.2015.06.007 . - DOI - PubMed
-
- Gremeaux V, Duclay J, Deley G, Philipp JL, Laroche D, Pousson M, et al. Does eccentric endurance training improve walking capacity in patients with coronary artery disease? A randomized controlled pilot study. Clin Rehabil. 2010;24(7):590–9. Epub 2010/06/10. doi: 10.1177/0269215510362322 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
