

Use of Magnetic Resonance Imaging in Neuroprognostication After Pediatric Cardiac Arrest: Survey of Current Practices
- PMID: 35835025
- PMCID: PMC9883065
- DOI: 10.1016/j.pediatrneurol.2022.06.011
Use of Magnetic Resonance Imaging in Neuroprognostication After Pediatric Cardiac Arrest: Survey of Current Practices
Abstract
Background: Use of magnetic resonance imaging (MRI) as a tool to aid in neuroprognostication after cardiac arrest (CA) has been described, yet details of specific indications, timing, and sequences are unknown. We aim to define the current practices in use of brain MRI in prognostication after pediatric CA.
Methods: A survey was distributed to pediatric institutions participating in three international studies. Survey questions related to center demographics, clinical practice patterns of MRI after CA, neuroimaging resources, and details regarding MRI decision support.
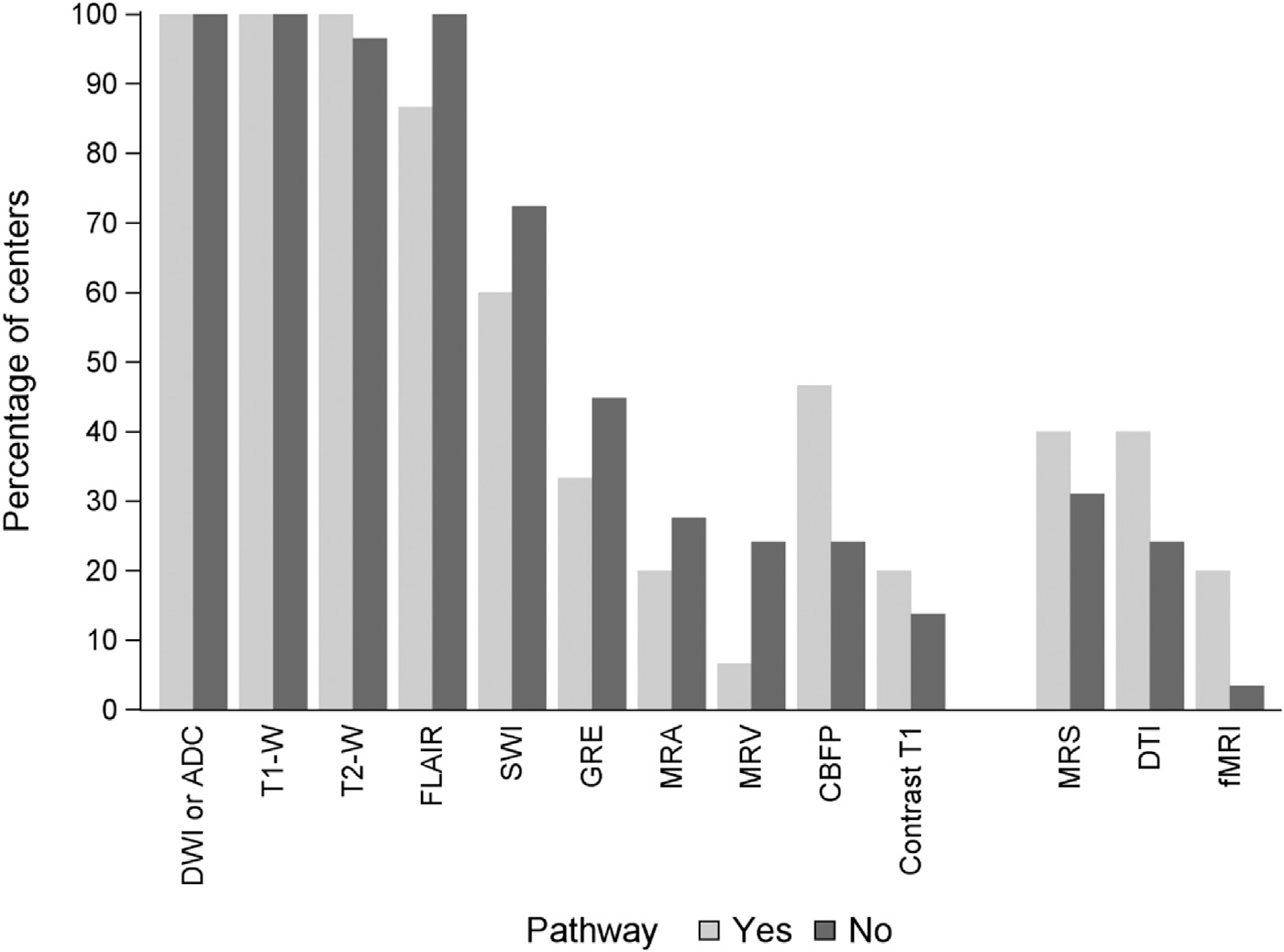
Results: Response rate was 31% (44 of 143). Thirty-four percent (15 of 44) of centers have a clinical pathway informing the use of MRI after CA. Fifty percent (22 of 44) of respondents reported that an MRI is obtained in nearly all patients with CA, and 32% (14 of 44) obtain an MRI in those who do not return to baseline neurological status. Poor neurological examination was reported as the most common factor (91% [40 of 44]) determining the timing of the MRI. Conventional sequences (T1, T2, fluid-attenuated inversion recovery, and diffusion-weighted imaging/apparent diffusion coefficient) are routinely used at greater than 97% of centers. Use of advanced imaging techniques (magnetic resonance spectroscopy, diffusion tensor imaging, and functional MRI) were reported by less than half of centers.
Conclusions: Conventional brain MRI is a common practice for prognostication after CA. Advanced imaging techniques are used infrequently. The lack of standardized clinical pathways and variability in reported practices support a need for higher-quality evidence regarding the indications, timing, and acquisition protocols of clinical MRI studies.
Keywords: Brain; Cardiac arrest; Child; Hypoxia-ischemia; MRI; Neuroimaging; Surveys and questionnaires.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declarations of Interest: Dr. Fink receives funding from National Institute of Neurological Disorders and Stroke (NINDS) R01NS096714 and Neurocritical Care Society Incline Grant.
Dr. Piantino receives support from the National Institute of Health, National Heart, Lung, and Blood Institute, grant K23HL150217.
Dr. Press has performed paid expert testimony and provides consulting for Marinus Pharmaceuticals.
The remaining authors have no relevant interests to disclose.
Figures
References
-
- Topjian AA, Berg RA. Pediatric out-of-hospital cardiac arrest. Circulation. 2012;125:2374–2378. - PubMed
-
- Knudson JD, Neish SR, Cabrera AG, et al. Prevalence and outcomes of pediatric in-hospital cardiopulmonary resuscitation in the United States: an analysis of the Kids’ Inpatient Database. Crit Care Med. 2012;40:2940–2944. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
