

Contributions of the Women's Health Initiative to Cardiovascular Research: JACC State-of-the-Art Review
- PMID: 35835498
- PMCID: PMC10324098
- DOI: 10.1016/j.jacc.2022.05.016
Contributions of the Women's Health Initiative to Cardiovascular Research: JACC State-of-the-Art Review
Abstract
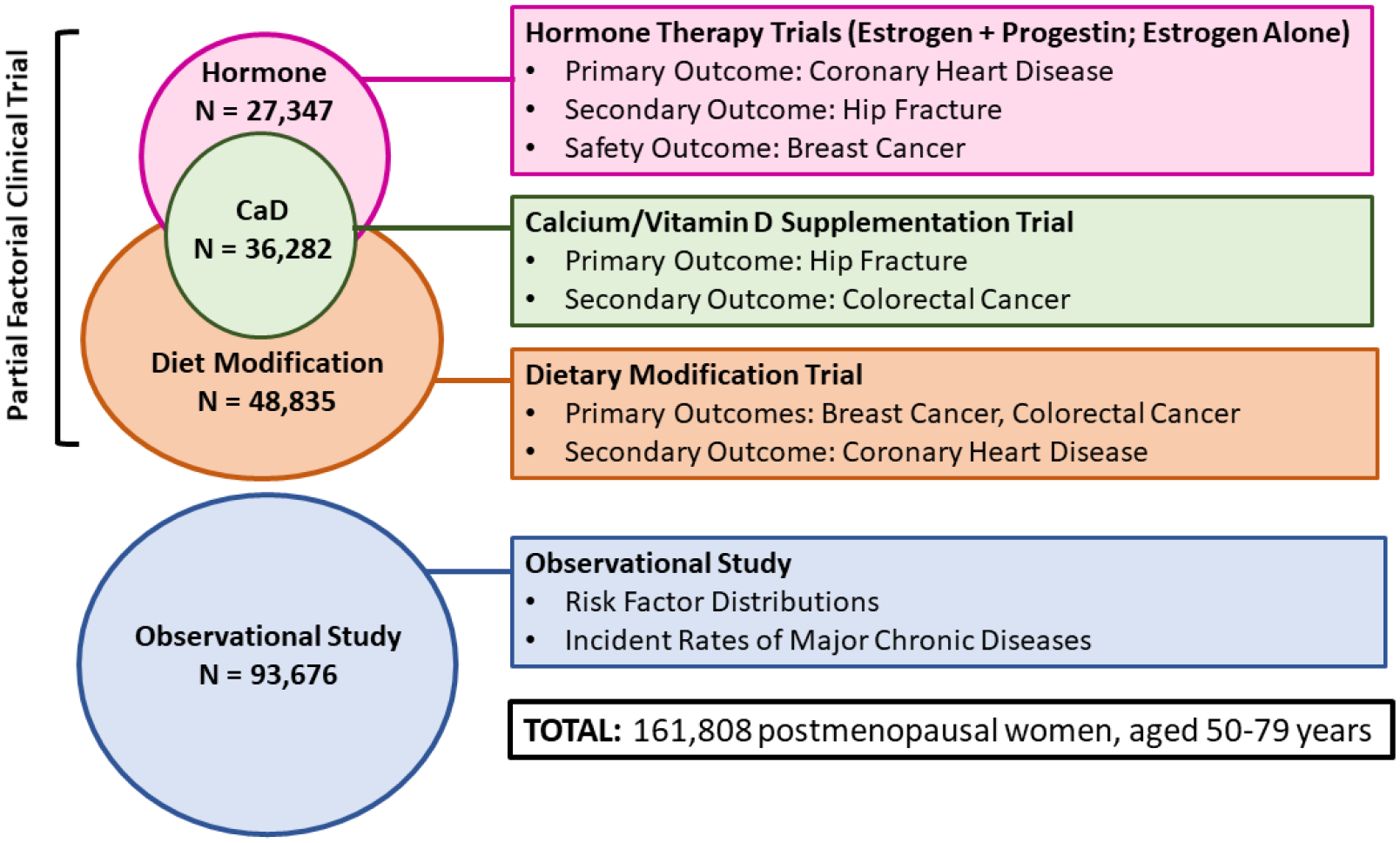
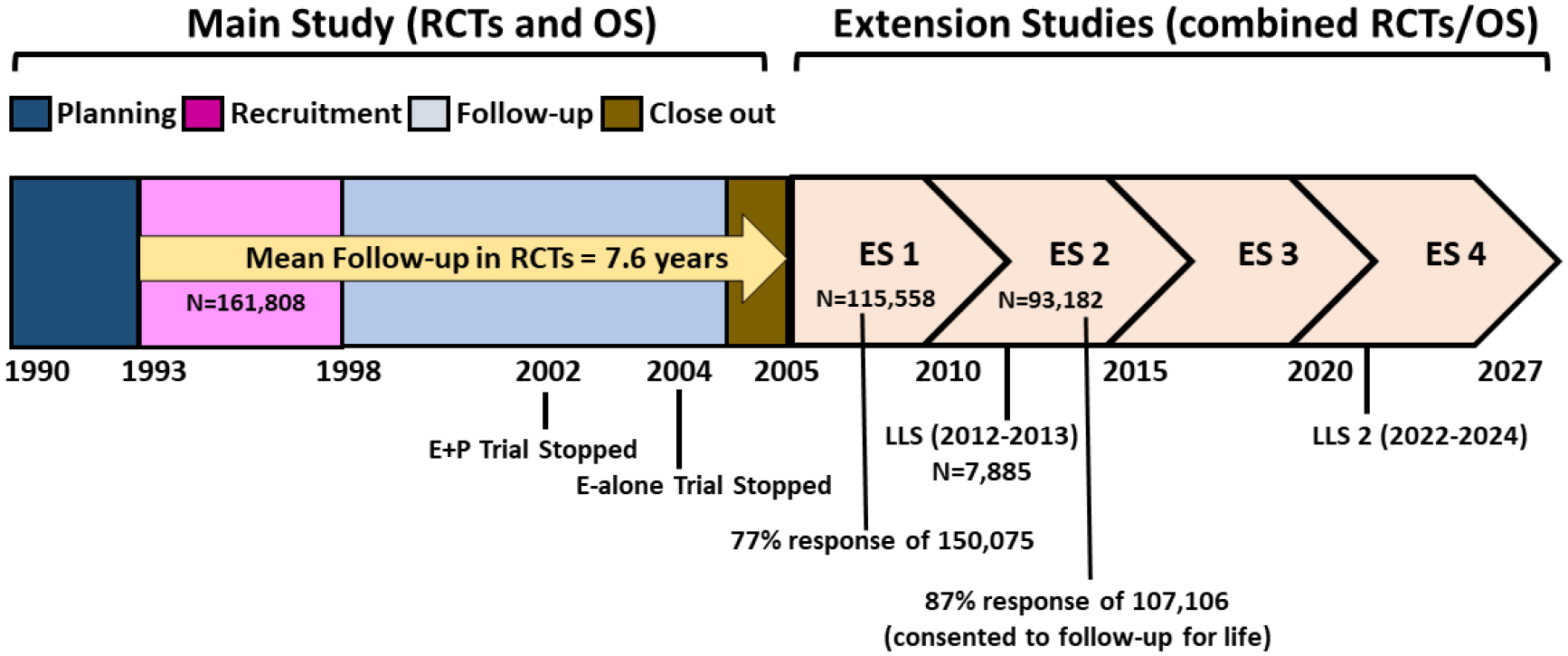
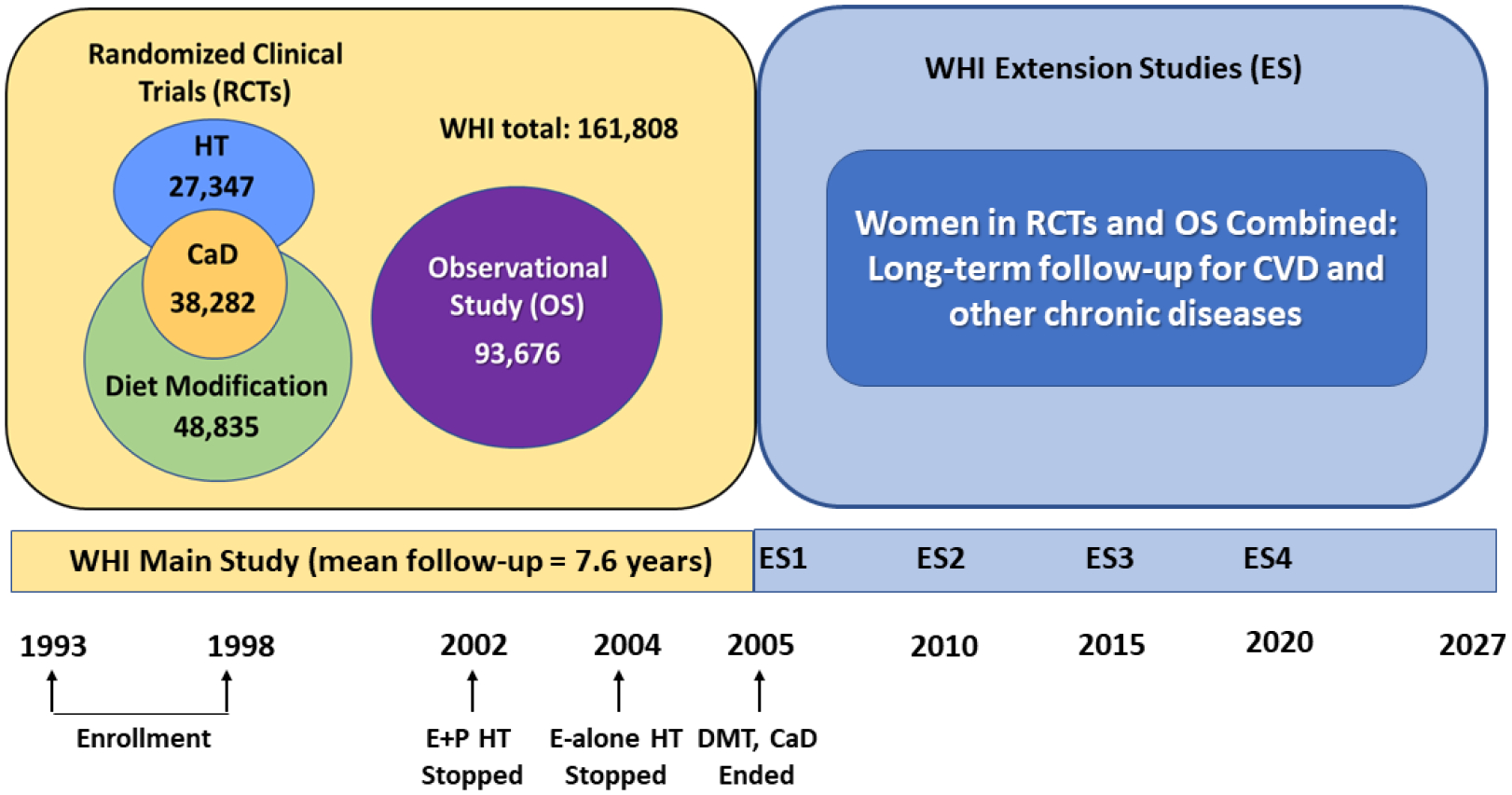
The WHI (Women's Health Initiative) enrolled 161,808 racially and ethnically diverse postmenopausal women, ages 50-79 years, from 1993 to 1998 at 40 clinical centers across the United States. In its clinical trial component, WHI evaluated 3 randomized interventions (menopausal hormone therapy; diet modification; and calcium/vitamin D supplementation) for the primary prevention of major chronic diseases, including cardiovascular disease, in older women. In the WHI observational study, numerous clinical, behavioral, and social factors have been evaluated as predictors of incident chronic disease and mortality. Although the original interventions have been completed, the WHI data and biomarker resources continue to be leveraged and expanded through ancillary studies to yield novel insights regarding cardiovascular disease prevention and healthy aging in women.
Keywords: cardiovascular disease; epidemiology; menopause; prevention; randomized trial; women’s health.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The WHI program is funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through contracts 75N92021D00001, 75N92021D00002, 75N92021D00003, 75N92021D0004, and 75N92021D00005; with additional funding by HL151885 (WHISH Trial), HL130591 (WHISH-2-Prevent Heart Failure), HL136398 (WHISH-STAR), HL150170 (Cross-Cohort Consortium Heart Failure), HL148565 (CHIP), HL133684 (WHISPER), HL105065 and HL153462 (OPACH), and AG050657 (COSMOS-Mind). The views expressed in this paper are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health; or the U.S. Department of Health and Human Services. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Department of Health and Human Services. Healy proposes historic Women’s Health Initiative. The NIH Reporter 1991;43:1, 4–5.
-
- Rossouw JE, Finnegan LP, Harlan WR, Pinn VW, Clifford C, McGowan JA. The evolution of the Women’s Health Initiative: perspectives from the NIH. J Am Med Womens Assoc 1995;50:50–5. - PubMed
-
- Design of the Women’s Health Initiative clinical trial and observational study. The Women’s Health Initiative Study Group. Controlled Clinical Trials 1998;19:61–109. - PubMed
-
- Hays J, Hunt JR, Hubbell FA et al. The Women’s Health Initiative recruitment methods and results. Annals Epidemiol 2003;13:S18–77. - PubMed
-
- Curb JD, McTiernan A, Heckbert SR et al. Outcomes ascertainment and adjudication methods in the Women’s Health Initiative. Annals Epidemiol 2003;13:S122–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 75N92021D00002/HL/NHLBI NIH HHS/United States
- R61 HL151885/HL/NHLBI NIH HHS/United States
- 75N92021D00005/WH/WHI NIH HHS/United States
- R01 HL130591/HL/NHLBI NIH HHS/United States
- R01 AG050657/AG/NIA NIH HHS/United States
- 75N92021D00001/HL/NHLBI NIH HHS/United States
- 75N92021D00003/WH/WHI NIH HHS/United States
- R33 HL151885/HL/NHLBI NIH HHS/United States
- R01 HL133684/HL/NHLBI NIH HHS/United States
- R01 HL153462/HL/NHLBI NIH HHS/United States
- R01 HL150170/HL/NHLBI NIH HHS/United States
- 75N92021D00004/WH/WHI NIH HHS/United States
- R01 HL105065/HL/NHLBI NIH HHS/United States
- R01 HL148565/HL/NHLBI NIH HHS/United States
- HHSN268201100046C/HL/NHLBI NIH HHS/United States
