

Use of Fluconazole-impregnated Beads to Treat Osteomyelitis Caused by Coccidioides in a Pigtailed Macaque (Macaca nemestrina)
- PMID: 35835541
- PMCID: PMC9413521
- DOI: 10.30802/AALAS-CM-21-000107
Use of Fluconazole-impregnated Beads to Treat Osteomyelitis Caused by Coccidioides in a Pigtailed Macaque (Macaca nemestrina)
Abstract
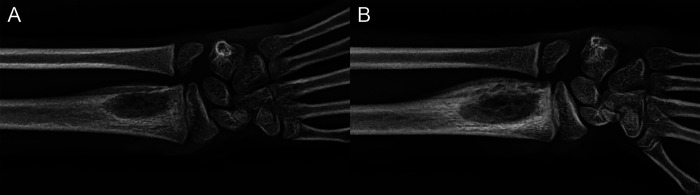
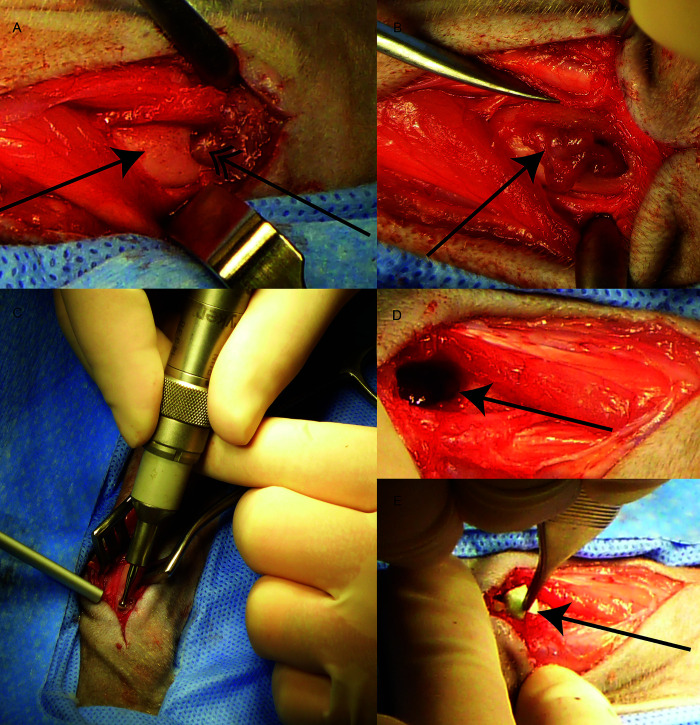
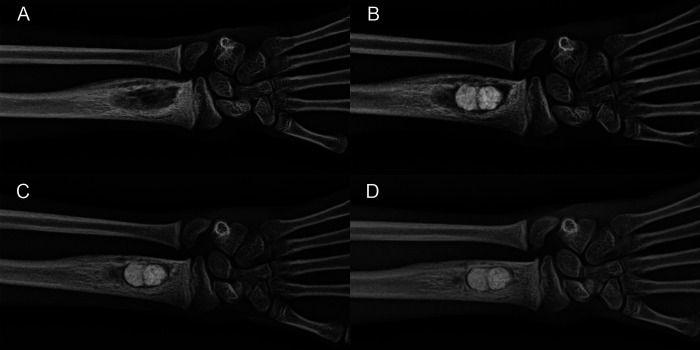
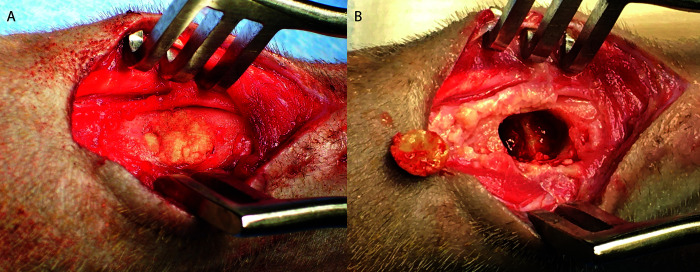
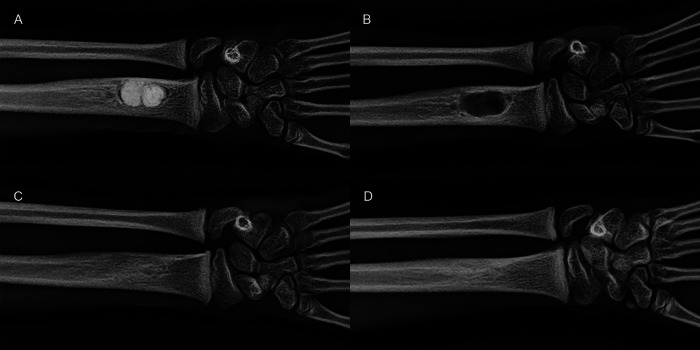
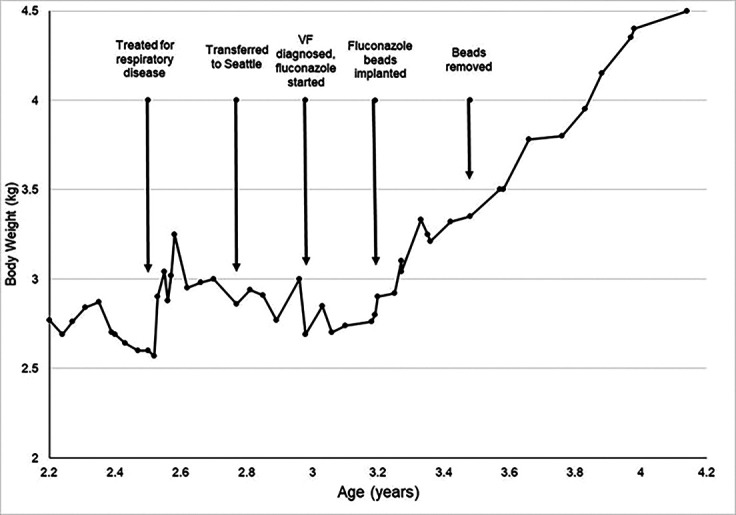
A 3-y-old male pigtailed macaque (Macaca nemestrina) presented for swelling of the left distal forearm and decreased use of the arm. The monkey had been raised at an indoor-outdoor facility in Arizona and transferred to an indoor facility in Washington 2 mo prior to presentation. A preliminary diagnosis of fungal osteomyelitis of the radius was made based on radiographs and Coccidioides titers. In addition to systemic antifungal treatment, surgery was performed to debride the bony lesion and implant polymethylmethacrylate beads impregnanted with the anti-fungal fluconazole. Histologic examination of the debrided material confirmed the diagnosis of fungal osteomyelitis. The surgical procedure resulted in clinical improvement, as evidenced by weight gain and decreased Coccidioides titers. The beads were removed in a second surgery, and the bony lesion completely resolved. With continued systemic fluconazole treatment, the monkey remained healthy with no further evidence of osteomyelitis. Coccidioides is an emerging pathogen that causes significant morbidity and mortality in both humans and animals. Bone infections can be resistant to systemic treatment, and the implantation of fluconazoleimpregnated beads may offer a successful treatment strategy for fungal osteomyelitis.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
