

Systematic Review of Cost-Effectiveness Analyses Comparing Open and Minimally Invasive Lumbar Spinal Surgery
- PMID: 35835570
- PMCID: PMC9421209
- DOI: 10.14444/8297
Systematic Review of Cost-Effectiveness Analyses Comparing Open and Minimally Invasive Lumbar Spinal Surgery
Abstract
Background: Minimally invasive surgery (MIS) has benefits over open surgery for lumbar decompression and/or fusion. Published literature on its cost-effectiveness vs open techniques is mixed.
Objective: Systematically review the cost-effectiveness of minimally invasive vs open lumbar spinal surgical decompression, fusion, or discectomy using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
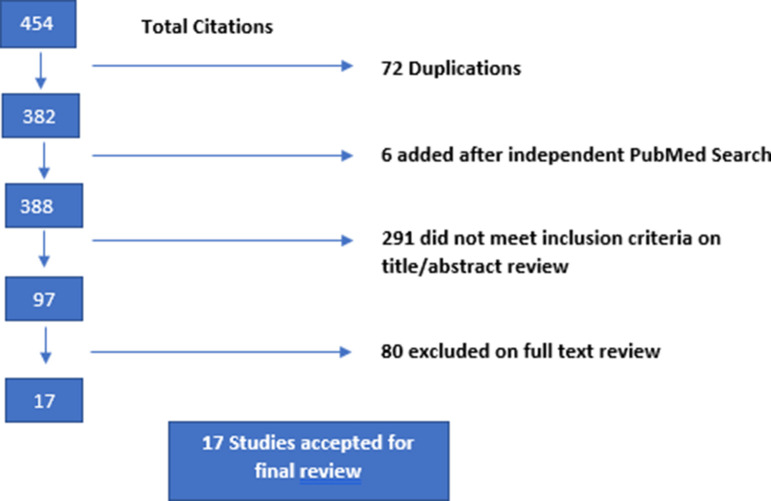
Methods: A systematic electronic search of databases (MEDLINE, Embase, and Cochrane Library) and a manual search from the cost-effectiveness analysis (CEA) database and National Health Service economic evaluation database was conducted. Studies that included adult populations undergoing surgery for degenerative changes in the lumbar spine (stenosis, radiculopathy, and spondylolisthesis) and reported outcomes of costing analysis, CEA, or incremental cost-effectiveness ratio were included.
Results: A total of 17 studies were included. Three studies assessed outcomes of MIS vs open discectomy. All 3 reported statistically significant lower total costs in the MIS, compared with the open group, with similar reported gains in quality-adjusted life years (QALYs). Two studies reported cost differences in MIS vs open laminectomy, with significantly lower total costs attributed to the MIS group. Twelve studies reported findings on the relative direct costs of MIS vs open lumbar fusion. Among those, 3 of the 4 studies comparing single-level MIS-transforaminal lumbar interbody fusion (TLIF) and open TLIF reported lower total costs associated with MIS procedures. Six studies reported cost evaluation of single- and 2-level TLIF procedures. Lower total costs were found in the MIS group compared with the open fusion group in all studies except for the subgroup analysis of 2-level fusions in a single study. Three of these 6 studies reported cost-effectiveness (cost/QALY). MIS fusion was found to be more cost-effective than open fusion in all 3 studies.
Conclusion: The studies reviewed were of poor to moderate methodological quality. Generally, studies reported a reduced cost associated with MIS vs open surgery and suggested better cost-effectiveness, particularly in MIS vs open single- and 2-level TLIF procedure. Most studies had a high risk of bias. Therefore, this review was unable to conclusively recommend MIS over open surgery from a cost-effectiveness perspective.
Clinical relevance: The incidence of spinal decompressive and fusion surgey and financial constraints on healthcare services continue to increase. This study aims to identify the cost and clinical effectiveness of common approaches to spinal surgery.
Level of evidence: 3a.
Keywords: QALY; QUALY; cost; cost-effectiveness; cost-minimization; cost-utility; discectomy; lumbar spine; minimal access surgery; minimally invasive; quality-adjusted life year; systematic review.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests: The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials