The hidden link between circadian entropy and mental health disorders
- PMID: 35835742
- PMCID: PMC9283542
- DOI: 10.1038/s41398-022-02028-3
The hidden link between circadian entropy and mental health disorders
Abstract
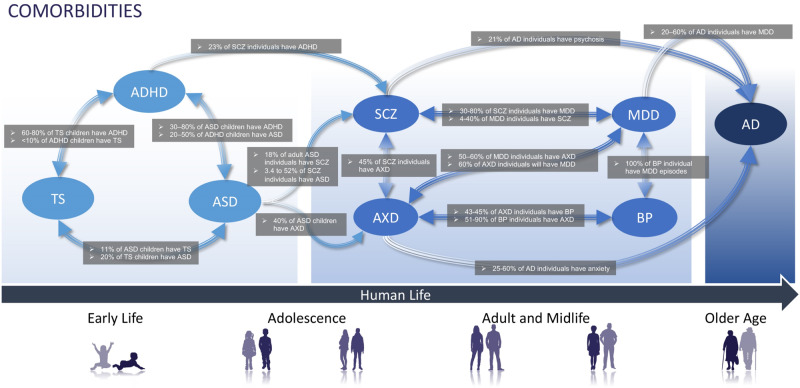
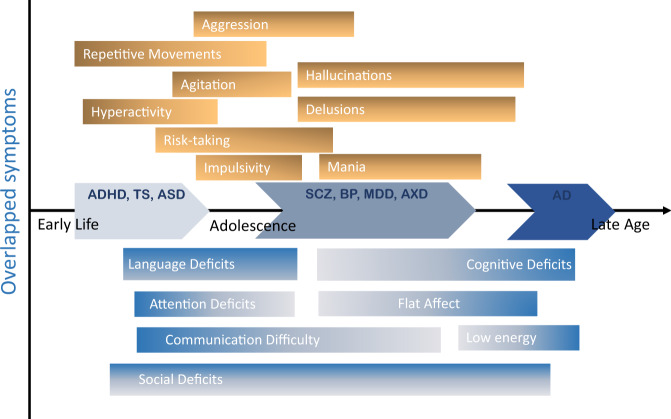
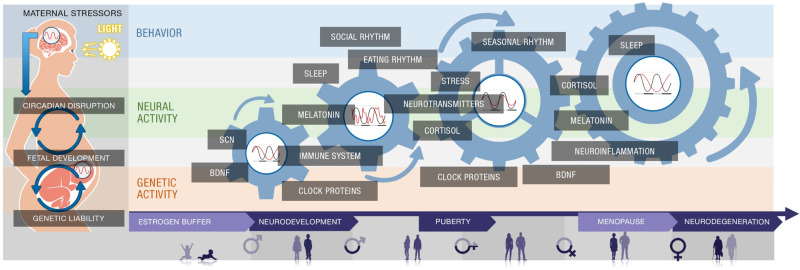
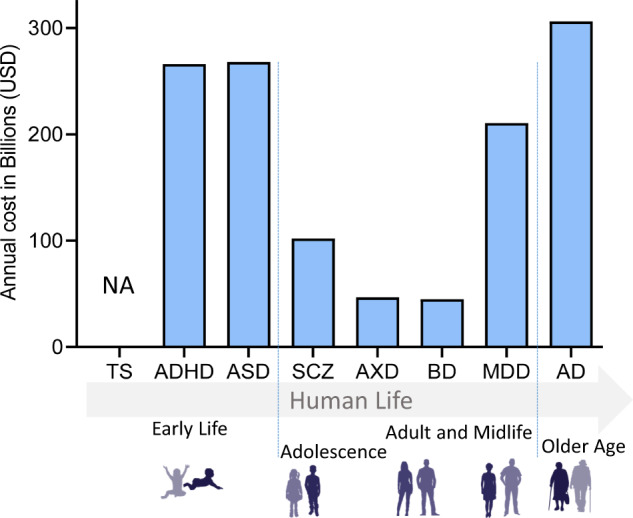
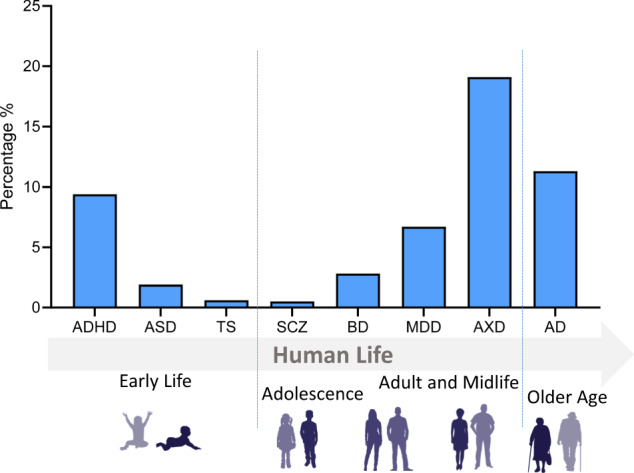
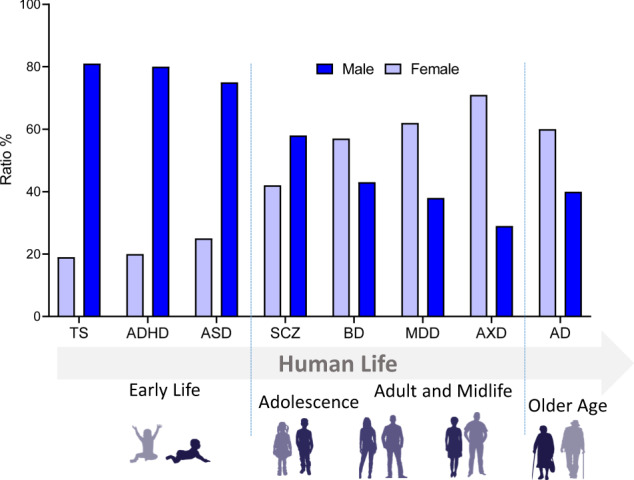
The high overlapping nature of various features across multiple mental health disorders suggests the existence of common psychopathology factor(s) (p-factors) that mediate similar phenotypic presentations across distinct but relatable disorders. In this perspective, we argue that circadian rhythm disruption (CRD) is a common underlying p-factor that bridges across mental health disorders within their age and sex contexts. We present and analyze evidence from the literature for the critical roles circadian rhythmicity plays in regulating mental, emotional, and behavioral functions throughout the lifespan. A review of the literature shows that coarse CRD, such as sleep disruption, is prevalent in all mental health disorders at the level of etiological and pathophysiological mechanisms and clinical phenotypical manifestations. Finally, we discuss the subtle interplay of CRD with sex in relation to these disorders across different stages of life. Our perspective highlights the need to shift investigations towards molecular levels, for instance, by using spatiotemporal circadian "omic" studies in animal models to identify the complex and causal relationships between CRD and mental health disorders.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures