

Multimorbidity
- PMID: 35835758
- PMCID: PMC7613517
- DOI: 10.1038/s41572-022-00376-4
Multimorbidity
Abstract
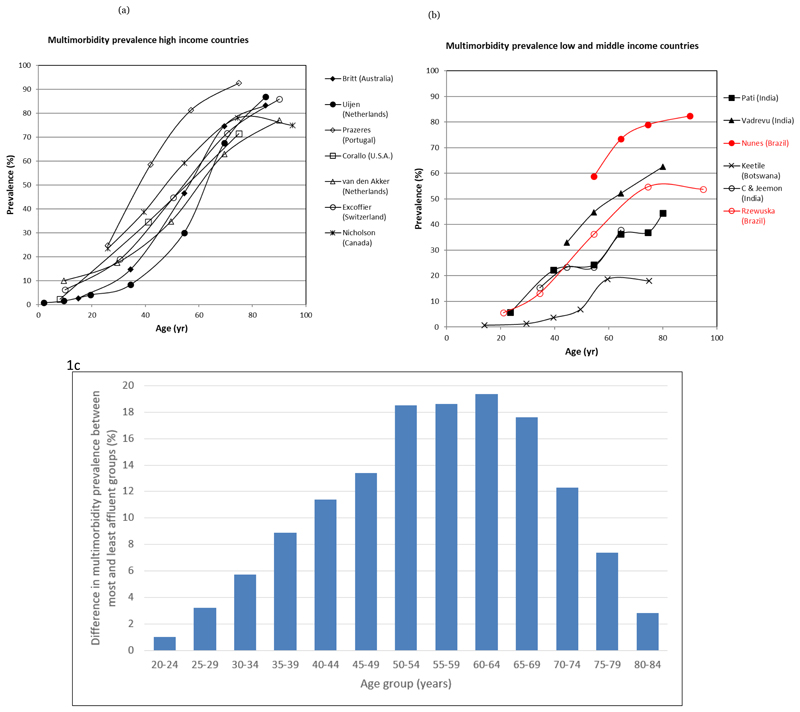
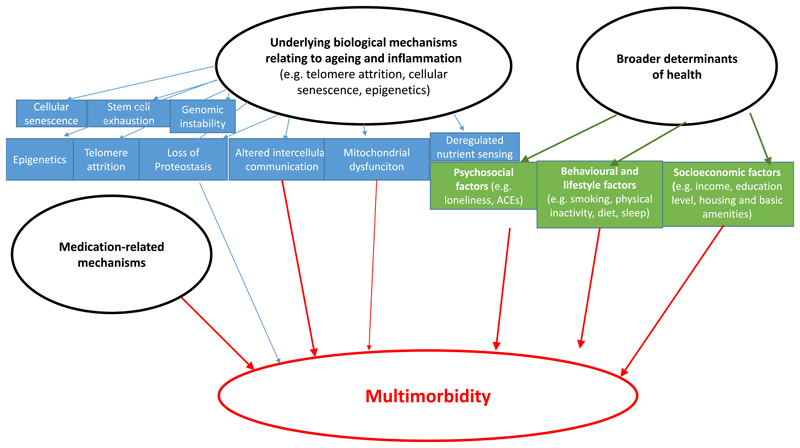
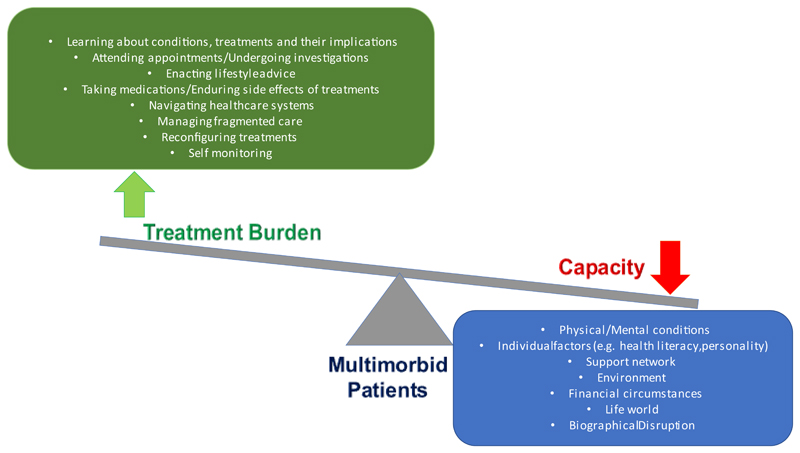
Multimorbidity (two or more coexisting conditions in an individual) is a growing global challenge with substantial effects on individuals, carers and society. Multimorbidity occurs a decade earlier in socioeconomically deprived communities and is associated with premature death, poorer function and quality of life and increased health-care utilization. Mechanisms underlying the development of multimorbidity are complex, interrelated and multilevel, but are related to ageing and underlying biological mechanisms and broader determinants of health such as socioeconomic deprivation. Little is known about prevention of multimorbidity, but focusing on psychosocial and behavioural factors, particularly population level interventions and structural changes, is likely to be beneficial. Most clinical practice guidelines and health-care training and delivery focus on single diseases, leading to care that is sometimes inadequate and potentially harmful. Multimorbidity requires person-centred care, prioritizing what matters most to the individual and the individual's carers, ensuring care that is effectively coordinated and minimally disruptive, and aligns with the patient's values. Interventions are likely to be complex and multifaceted. Although an increasing number of studies have examined multimorbidity interventions, there is still limited evidence to support any approach. Greater investment in multimorbidity research and training along with reconfiguration of health care supporting the management of multimorbidity is urgently needed.
© 2022. Springer Nature Limited.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

References
-
- Atun R. Transitioning health systems for multimorbidity. Lancet (London, England) 2015;386:721–722. - PubMed
Publication types
MeSH terms
Grants and funding
- 074833/Z/04/Z/WT_/Wellcome Trust/United Kingdom
- NIHR203986/DH_/Department of Health/United Kingdom
- MC_PC_MR/T037849/1/MRC_/Medical Research Council/United Kingdom
- MR/P024408/1/MRC_/Medical Research Council/United Kingdom
- U01 HL114180/HL/NHLBI NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- D71 TW010877/TW/FIC NIH HHS/United States
- NIHR202644/DH_/Department of Health/United Kingdom
- P30 AG066587/AG/NIA NIH HHS/United States
- UM1 HL134590/HL/NHLBI NIH HHS/United States
- 107435/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MR/T037849/1/MRC_/Medical Research Council/United Kingdom
- P20 CA217231/CA/NCI NIH HHS/United States
- 218743/Z/19/Z/WT_/Wellcome Trust/United Kingdom
- BB/T009004/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- NIHR202020/DH_/Department of Health/United Kingdom
- MR/P008984/1/MRC_/Medical Research Council/United Kingdom
- 103994/Z/14/Z/WT_/Wellcome Trust/United Kingdom
- HHSN268200900033C/HL/NHLBI NIH HHS/United States
- R21 TW011740/TW/FIC NIH HHS/United States
- 205177/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 214185/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- R21 TW009982/TW/FIC NIH HHS/United States
- R24 AG064025/AG/NIA NIH HHS/United States
- MR/P02386X/1/MRC_/Medical Research Council/United Kingdom
- K24 AG056578/AG/NIA NIH HHS/United States
- MR/M007405/1/MRC_/Medical Research Council/United Kingdom
- U19 MH098780/MH/NIMH NIH HHS/United States
- 801790/ERC_/European Research Council/International
- 093541/Z/10/Z/WT_/Wellcome Trust/United Kingdom
- MR/T03775X/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
