

Border tissue morphology is associated with the pattern of visual field progression in open-angle glaucoma
- PMID: 35835923
- PMCID: PMC9283464
- DOI: 10.1038/s41598-022-16186-3
Border tissue morphology is associated with the pattern of visual field progression in open-angle glaucoma
Abstract
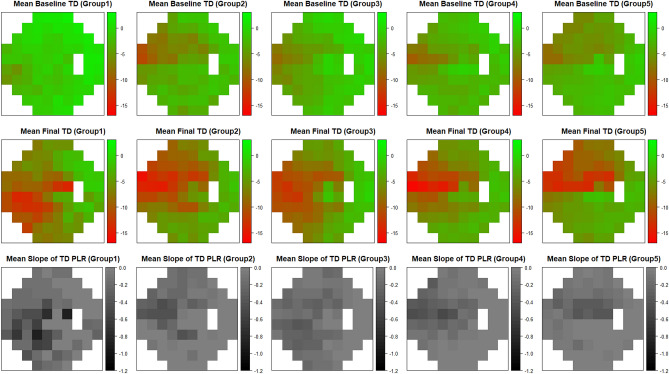
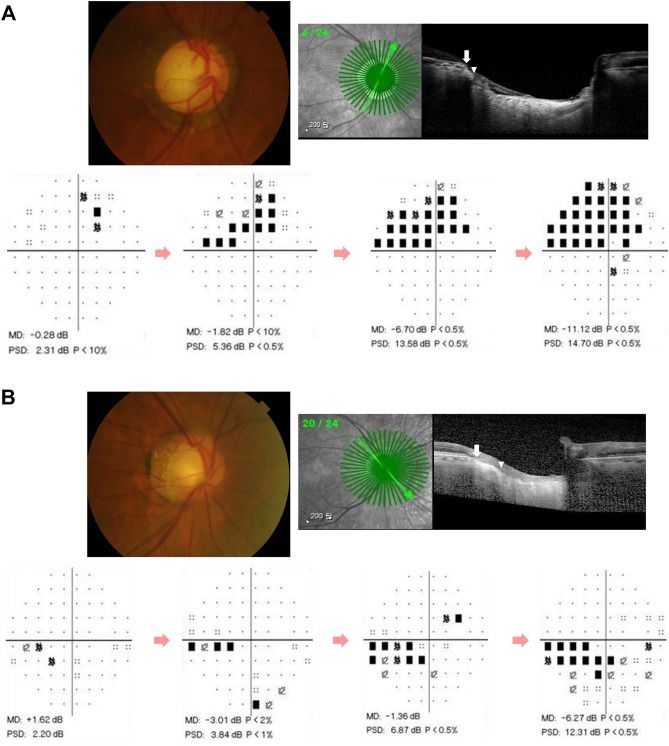
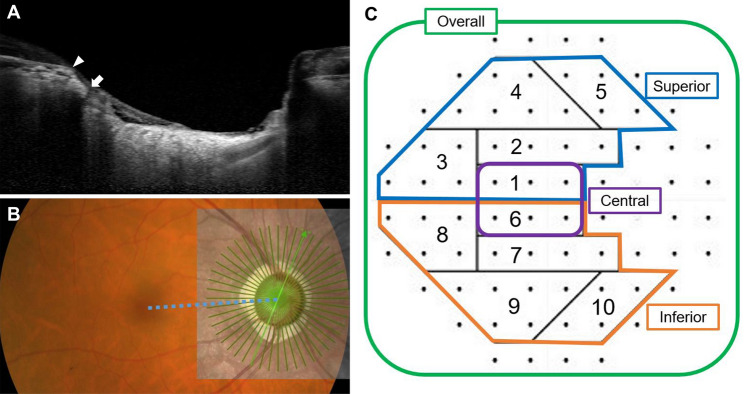
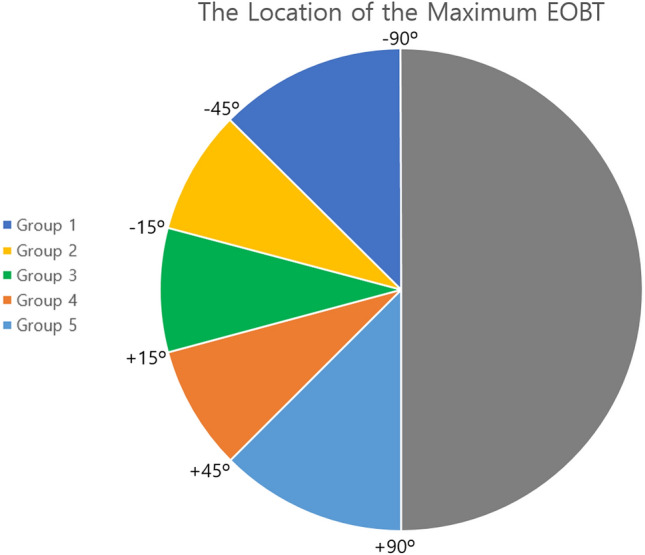
The etiology of open-angle glaucoma (OAG) is yet unclear. This study investigated possible risk factors, such as the morphology of the border tissue that affect the pattern of visual field (VF) progression in eyes with OAG. 166 eyes of 166 OAG patients with an externally oblique border tissue (EOBT) at least in one direction were included. EOBT was obtained by analyzing enhanced depth imaging spectral-domain optical coherence tomography images. A pointwise linear regression was used to determine VF progression by measuring the deterioration rate of each point in the VF. The odds ratio of VF progression for each risk factor was estimated using logistic regression analysis. Seventy (42.2%) eyes showed VF deterioration. In multivariate analysis, longer follow-up period, higher baseline intraocular pressure (IOP), lower mean ocular perfusion pressure (MOPP), and smaller angular location of the longest EOBT were associated with VF progression (all p values were below 0.05). In the multivariate analysis, the location of the longest EOBT was significantly associated with inferior (p = 0.002) and central (p = 0.017) VF progression. In conclusion, VF progression pattern in OAG eyes is associated with the location of the longest EOBT as well as other known risk factors.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Deep Optic Nerve Head Morphology Is Associated With Pattern of Glaucomatous Visual Field Defect in Open-Angle Glaucoma.Invest Ophthalmol Vis Sci. 2018 Aug 1;59(10):3842-3851. doi: 10.1167/iovs.18-24588. Invest Ophthalmol Vis Sci. 2018. PMID: 30073358
-
Border Tissue Morphology Is Spatially Associated with Focal Lamina Cribrosa Defect and Deep-Layer Microvasculature Dropout in Open-Angle Glaucoma.Am J Ophthalmol. 2019 Jul;203:89-102. doi: 10.1016/j.ajo.2019.02.023. Epub 2019 Feb 28. Am J Ophthalmol. 2019. PMID: 30825418
-
An Increased Choroidal Microvasculature Dropout Size is Associated With Progressive Visual Field Loss in Open-Angle Glaucoma.Am J Ophthalmol. 2021 Mar;223:205-219. doi: 10.1016/j.ajo.2020.10.018. Epub 2020 Oct 28. Am J Ophthalmol. 2021. PMID: 33129811
-
Optic disc tilt direction affects regional visual field progression rates in myopic eyes with open-angle glaucoma.Graefes Arch Clin Exp Ophthalmol. 2016 Nov;254(11):2267-2276. doi: 10.1007/s00417-016-3501-0. Epub 2016 Oct 6. Graefes Arch Clin Exp Ophthalmol. 2016. PMID: 27714512
-
Baseline Choroidal Microvasculature Dropout as a Predictor of Subsequent Visual Field Progression in Open-angle Glaucoma.J Glaucoma. 2021 Aug 1;30(8):672-681. doi: 10.1097/IJG.0000000000001853. J Glaucoma. 2021. PMID: 33867502
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
