

Prevalence and treatment of fragility fractures in Spanish primary care: PREFRAOS study
- PMID: 35836031
- PMCID: PMC9283348
- DOI: 10.1007/s11657-022-01124-7
Prevalence and treatment of fragility fractures in Spanish primary care: PREFRAOS study
Abstract
In Spanish primary care (PC), the prevalence of fragility fractures (FF) in subjects ≥ 70 years old is high, especially in women. One-third of subjects with an FF lacked osteoporosis (OP) diagnosis and >50% were not currently receiving OP medication. An improvement of the FF management in this population is needed.
Purpose: In Spanish PC, the prevalence of FF is high, especially in women. One-third of subjects with a FF lacked an OP diagnosis and more than half were not currently receiving OP medication. Several studies reported underdiagnosis/undertreatment of OP in PC among elderly subjects with FF. To date, no such data exist for Spain. The purpose is to estimate the prevalence of FF in the elderly population (≥ 70 years old) and to describe the characteristics, risk factors, comorbidities, and OP diagnosis and treatment rates of subjects with FF in Spanish PC centers.
Methods: This is an observational, retrospective study in Spain consisting of two phases. Phase A included all subjects ≥ 70 years old listed in the center's medical records from November 2018 to March 2020. Phase B included subjects with FF and prior consultation at the center for any reason. Subjects were excluded only if they had previously participated in another study. Primary outcomes were prevalence of FF (phase A) and characteristics of subjects with at least one FF (phase B).
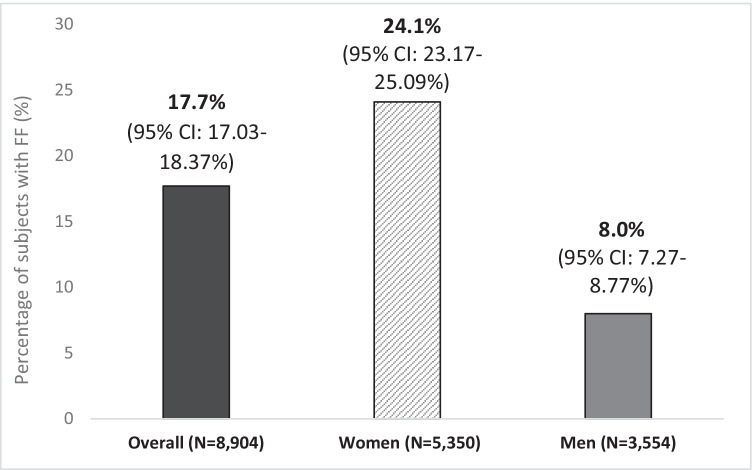
Results: The overall prevalence of FF was 17.7% among subjects visiting medical centers for any reason (24.1% women vs. 8.0% men) (30 PC centers from 14 Spanish regions). Vertebral (5.1%) was the most prevalent fracture. Of 665 subjects in phase B, most (87%) were women and ≥ 80 years old (57%), suffered mainly major OP fracture (68%), and had multiple comorbidities (≥ 2, 89.2%). While two-thirds had OP diagnosis and 61.1% received OP medication anytime in the past, 56.8% were not currently receiving OP medication. Diagnosis and treatment rates were lower among men (43% and 38% vs. 70% and 65%, respectively).
Conclusion: Prevalence of FF was high, especially in women. One-third of subjects lacked OP diagnosis and ≥ 50% were not receiving OP treatment; diagnosis and treatment gaps were larger among men. This reinforces the need to improve the management of FF in the elderly population. However, as PC centers participating in this study had high OP experience that have the potential to do better in terms of diagnosis and treatment, caution in the generalization of these data should be taken.
Keywords: Diagnostic; Fragility fracture; Osteoporosis; Prevalence; Primary care; Treatment.
© 2022. The Author(s).
Conflict of interest statement
DML: personal fees from Amgen, Lilly, Rubió, Gedeon Richter, Pierre Fabre, Grünenthal, Theramex, and Italfarmaco; JCB: personal fees from AstraZeneca, Esteve, Boehringer Ingelheim, Bayer, Abbott, Almirall, Amgen, Chiessi, FAES, Grunenthal, GSK, Lilly, Menarini, MSD, Pfizer, Recordatti, Rovi, and Servier; MG: personal fees from Amgen, Stada, Rubió, and Grünenthal; RMP: fees from Amgen, UCB, Stada, Angelini, and Gebro; FV: personal fees from Pfizer, Grünenthal, MSD, Amgen, GSK, Lilly, Bristol-Myers Squibb, Servier, P&G Pharmaceuticals, Novartis, Almirall, Sanofi, and Mundipharma; MB and LC: Amgen employees.
Figures

References
-
- Neustadt J (2013) Osteoporosis: beyond bone mineral density to maximize fracture reduction. Anti-Aging Therapeutics - 2012 Conference Year 121–38
-
- Bougioukli S, Κollia P, Koromila T, Varitimidis S, Hantes M, Karachalios T, et al. Failure in diagnosis and under-treatment of osteoporosis in elderly patients with fragility fractures. J Bone Miner Metab. 2018;17:37. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
