

An economic evaluation of cabazitaxel versus a second androgen receptor-targeted agent (ARTA) for patients with metastatic castration-resistant prostate cancer previously treated with docetaxel and an ARTA: the United States payer perspective
- PMID: 35836170
- PMCID: PMC9284907
- DOI: 10.1186/s12913-022-08274-x
An economic evaluation of cabazitaxel versus a second androgen receptor-targeted agent (ARTA) for patients with metastatic castration-resistant prostate cancer previously treated with docetaxel and an ARTA: the United States payer perspective
Abstract
Background: Cabazitaxel significantly improves clinical outcomes compared with a second androgen receptor-targeted agent (ARTA) in patients with metastatic castration-resistant prostate cancer (mCRPC) previously treated with docetaxel and an ARTA (abiraterone or enzalutamide), as demonstrated in the CARD trial (NCT02485691). We aimed to estimate healthcare costs avoided with the use of cabazitaxel as a third-line (3 L) treatment versus a second ARTA from a US payer perspective.
Methods: Model inputs were based on the CARD trial, published sources, and estimates of typical clinical care patterns by genitourinary oncologists (n = 3). Assessed time points were 6, 12, 18, and 24 months. Outcomes included progression-free survival (PFS), radiographic PFS (rPFS), and overall survival (OS); hospitalization and intensive care unit (ICU) days; and costs (reported in 2020 US dollar [USD] and converted into Euro) to manage symptomatic skeletal events (SSEs), adverse events (AEs), and end-of-life care.
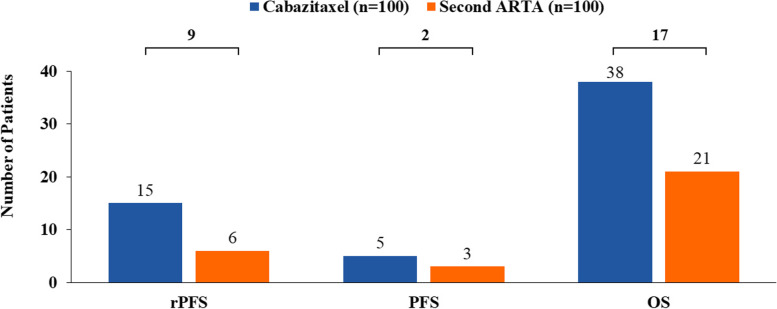
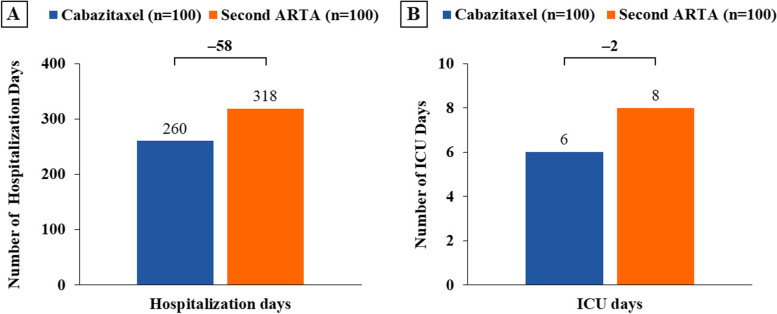
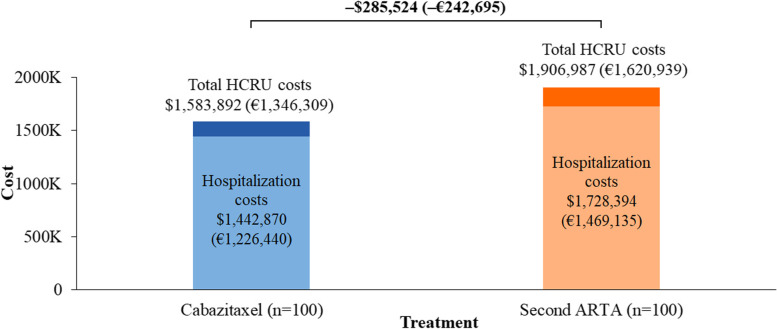
Results: At 18 months, in a cohort of 100 patients, the use of cabazitaxel was estimated to result in 9 more patients achieving rPFS, 2 more patients achieving PFS, and 17 more survivors versus a second ARTA. The costs of SSEs, AEs, and end-of-life care were $498,909 (€424,073), $276,198 (€234,768), and $808,785 (€687,468), respectively, for cabazitaxel and $627,569 (€533,434), $251,124 (€213,455), and $1,028,294 (€874,050), respectively, for a second ARTA. Cabazitaxel was estimated to be associated with a 21% reduction in both SSE management and end-of-life care costs. Hospitalization cost was $1,442,870 (€1,226,440) for cabazitaxel and $1,728,394 (€1,469,135) for a second ARTA, representing an estimated 17% reduction in these costs. Cabazitaxel, as compared with a second ARTA, was associated with 58 fewer hospitalization days and 2 fewer ICU days and was estimated to avoid $323,095 (€274,630, 17%) in total costs, driven by SSEs management and end-of-life care.
Conclusion: The use of cabazitaxel as a 3 L treatment after docetaxel and an ARTA in patients with mCRPC is estimated to result in clinical benefits (longer rPFS, PFS, and OS) and lower healthcare resource utilization (fewer hospitalization and ICU days), compared with a second ARTA.
Keywords: Androgen receptor-targeted agent; Cabazitaxel; Economic impact; End-of-life care; Metastatic castration-resistant prostate cancer; Symptomatic skeletal events; Third-line treatment.
© 2022. The Author(s).
Conflict of interest statement
AKM reported receiving honoraria and advisory fees from Genentech, AstraZeneca, Sanofi, Bayer, Astellas Pharma, Janssen, Advanced Accelerator Applications, Myovant Sciences, and Exelixis; advisory fees from Blue Earth Diagnostics; honoraria from Astellas Scientific and Medical Affairs Inc., Janssen Oncology, Clovis Oncology, and Pfizer; grant support from Astellas Scientific and Medical Affairs Inc., Bayer, Seattle Genetics/Astellas, Genentech, and AstraZeneca; and travel support from Sanofi. TH reports receiving honoraria, advisory fees, grant support, and fees for serving on a speaker’s bureau from Pfizer, Johnson & Johnson, Bristol-Myers Squibb, Eisai, and Exelixis; honoraria, advisory fees, and fees for serving on a speakers bureau from Astellas Pharma; and honoraria and advisory fees from Novartis and Bayer/Onyx. AKG reported being employed by EVERSANA and holding stock in Tyme Technologies and Area Biopharma. DG and AZ reported being employed by EVERSANA. ED reported being employed by and holding stock in Sanofi. NJV reported being employed by and receiving travel and grant support from US Oncology; advisory fees, travel support, and fees for serving on a speakers bureau from Bayer, Genentech/Roche, and AstraZeneca; advisory fees and fees for serving on a speakers bureau from Clovis Oncology and Myovant Sciences; advisory fees, travel support, and honoraria from Pfizer; honoraria and fees for serving as an expert testimony from Novartis; advisory fees, grant support, and honoraria from Merck; travel support and fees for serving on a speakers bureau from Sanofi; advisory fees and holding stock in Caris Life Sciences; advisory fees from Tolero Pharmaceuticals, Astellas Pharma, Boehringer Ingelheim, Corvus Pharmaceuticals, Modra Pharmaceuticals, Janssen Oncology, and Eisai; fees for serving on a speakers bureau from Bristol-Myers Squibb, Seattle Genetics/Astellas. and AVEO; travel support from Exelixis; honoraria from UpToDateand; grant support from Endocyte and Suzhou Kintor Pharmaceuticals. No other potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Baseline neutrophil-to-lymphocyte ratio as a predictive and prognostic biomarker in patients with metastatic castration-resistant prostate cancer treated with cabazitaxel versus abiraterone or enzalutamide in the CARD study.ESMO Open. 2021 Oct;6(5):100241. doi: 10.1016/j.esmoop.2021.100241. Epub 2021 Aug 24. ESMO Open. 2021. PMID: 34450475 Free PMC article. Clinical Trial.
-
Comparison of Sequential Treatment With Androgen Receptor-Targeted Agent Followed by Another Androgen Receptor-Targeted Agent Versus Androgen Receptor-Targeted Agent Followed by Docetaxel in Chemotherapy-Naive Patients With Metastatic Castration-Resistant Prostate Cancer.Clin Genitourin Cancer. 2017 Dec;15(6):e1073-e1080. doi: 10.1016/j.clgc.2017.07.016. Epub 2017 Jul 26. Clin Genitourin Cancer. 2017. PMID: 28826931
-
Real-world evidence of patients with metastatic castration-resistant prostate cancer treated with cabazitaxel: comparison with the randomized clinical study CARD.Prostate Cancer Prostatic Dis. 2023 Mar;26(1):67-73. doi: 10.1038/s41391-021-00487-1. Epub 2022 Jan 17. Prostate Cancer Prostatic Dis. 2023. PMID: 35039605 Free PMC article. Clinical Trial.
-
Real-World Cabazitaxel Use and Outcomes in Metastatic Castrate-Resistant Prostate Cancer: The Impact of Response to First ARPI.Clin Genitourin Cancer. 2022 Oct;20(5):496.e1-496.e9. doi: 10.1016/j.clgc.2022.04.009. Epub 2022 Apr 26. Clin Genitourin Cancer. 2022. PMID: 35599196 Review.
-
[Advanced prostate cancer: sequence of androgen receptor-targeted substances and chemotherapy determines long-term survival].Urologe A. 2021 Feb;60(2):212-221. doi: 10.1007/s00120-020-01411-6. Epub 2020 Dec 21. Urologe A. 2021. PMID: 33346857 Review. German.
References
-
- American Cancer Society: Cancer facts & figures 2020. Estimated number of new cancer cases and deaths by sex, US, 2020.[https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-...].
-
- Tamada S, Iguchi T, Kato M, Asakawa J, Kita K, Yasuda S, Yamasaki T, Matsuoka Y, Yamaguchi K, Matsumura K, et al. Time to progression to castration-resistant prostate cancer after commencing combined androgen blockade for advanced hormone-sensitive prostate cancer. Oncotarget. 2018;9(97):36966–36974. doi: 10.18632/oncotarget.26426. - DOI - PMC - PubMed
-
- de Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP, Kocak I, Gravis G, Bodrogi I, Mackenzie MJ, Shen L, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet. 2010;376(9747):1147–1154. doi: 10.1016/S0140-6736(10)61389-X. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
