

Temperature processing and distribution in larynx thermal inhalation injury with analogy to human airway cells: a mechanism of protection
- PMID: 35836876
- PMCID: PMC9274606
Temperature processing and distribution in larynx thermal inhalation injury with analogy to human airway cells: a mechanism of protection
Abstract
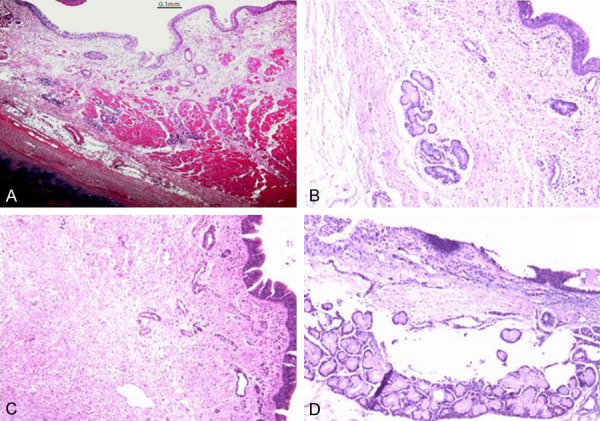
Objective: Inhalation injuries, especially laryngeal injuries, threaten the lives of burn patients. Unlike studies on temperature distribution in the upper airway, studies on temperature development in different laryngeal layers, including the mucosa, lamina propria, cartilage, muscle, and subcutaneous layer, are lacking.
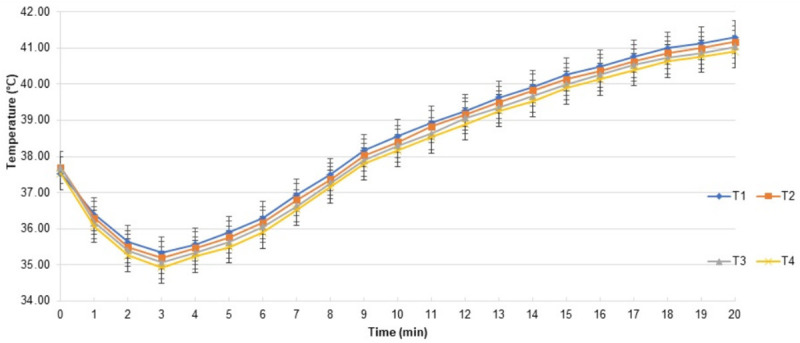
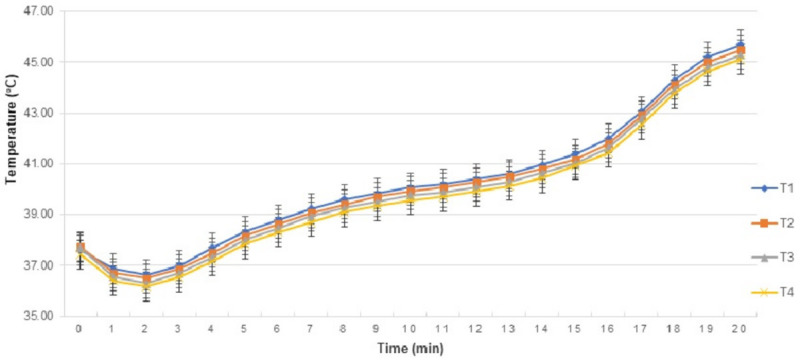
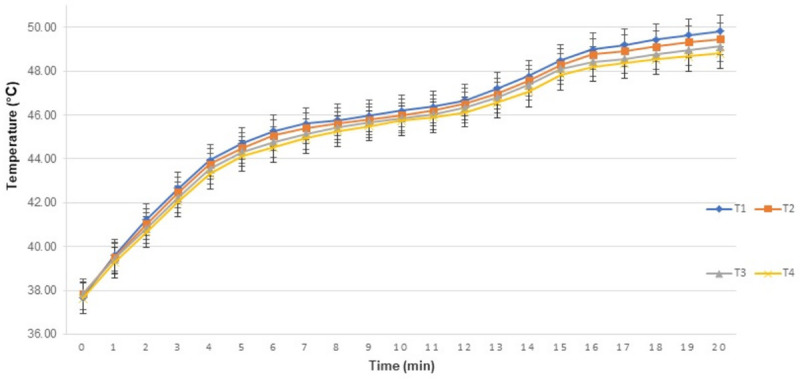
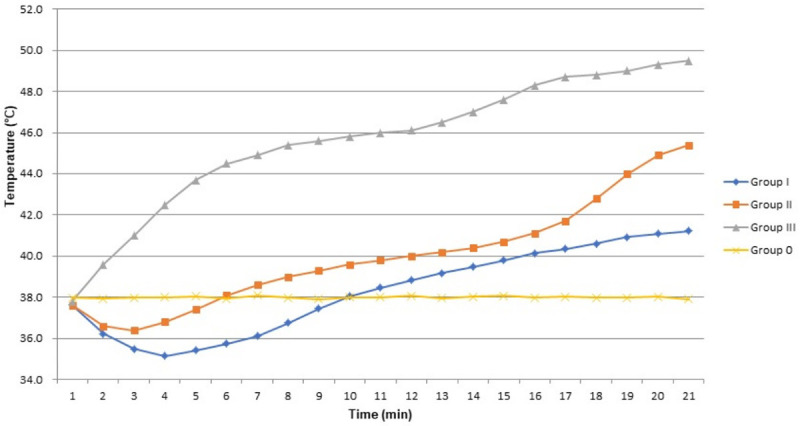
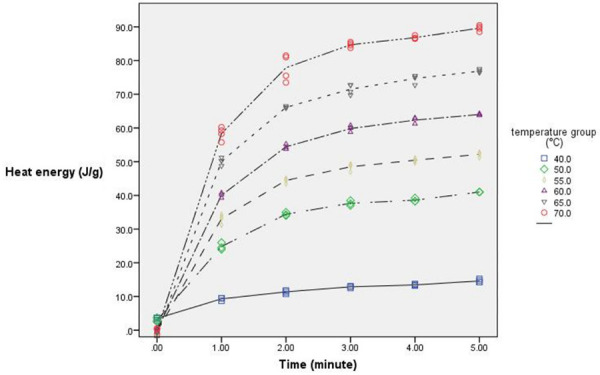
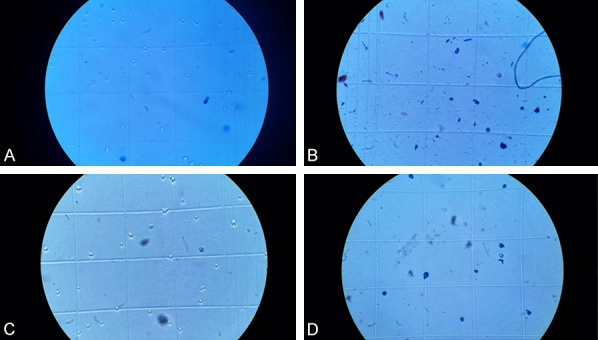
Method: For the in-vivo study, 16 healthy adult male beagles were divided into four groups: control, low-, medium-, and high-heat groups, inhaling dry air at 26, 80, 160, and 320°C for 20 min, with temperature probes punctured through skin into layers as mentioned, and heat energy was calculated. For the in-vitro study, we heated human lung fibroblasts and bronchial epithelial cells using a similar heating profile with heat energy of 15-90 J/g to investigate cell survival and viability for clinical comparison.
Results: No statistical difference emerged between the temperatures of different laryngeal layers at each timepoint. The temperatures decreased significantly and shortly before increasing unevenly in the low- and medium-heat groups. The survival rates and viability of the two cell lines correlated negatively with heat energy. The heat energy absorbed in the low-, medium-, and high-heat groups of beagles were 12, 29, and 44 J/g, with calculated in-vitro human cell survival rates of 114%, 90%, and 69%, respectively, for the corresponding energy levels.
Conclusions: The abnormal temperature processing and lack of a difference between layers indicate an effective self-protective mechanism of heat conduction in larynx. The in-vitro results demonstrate a high survival rate of lung cells at comparable heat energy levels to those measured in the larynx.
Keywords: Inhalation injury; heat tolerance; larynx.
AJTR Copyright © 2022.
Conflict of interest statement
None.
Figures
Similar articles
-
Protection of laryngeal mucosa and function in laryngeal burns by heat absorption of perilaryngeal tissue.Eur Arch Otorhinolaryngol. 2023 Oct;280(10):4531-4542. doi: 10.1007/s00405-023-08030-9. Epub 2023 May 23. Eur Arch Otorhinolaryngol. 2023. PMID: 37219683
-
Temperature distribution in the upper airway after inhalation injury.Burns. 2011 Nov;37(7):1187-91. doi: 10.1016/j.burns.2011.06.004. Epub 2011 Aug 3. Burns. 2011. PMID: 21816541
-
[Morphological and pathological changes of larynx after severe laryngeal burn in dogs and their relationship with laryngostenosis].Zhonghua Shao Shang Za Zhi. 2018 Aug 20;34(8):549-555. doi: 10.3760/cma.j.issn.1009-2587.2018.08.013. Zhonghua Shao Shang Za Zhi. 2018. PMID: 30157560 Chinese.
-
The effects of excessive humidity.Respir Care Clin N Am. 1998 Jun;4(2):215-28. Respir Care Clin N Am. 1998. PMID: 9648183 Review.
-
Blood flow rate, temperature, oxygen tension and consumption in the skin of adults measured by a heated microcathode oxygen electrode.Dan Med Bull. 1988 Aug;35(4):322-34. Dan Med Bull. 1988. PMID: 3048920 Review.
Cited by
-
Effect of continuous local dexamethasone on tissue biomechanics and histology after inhalational burn in a preclinical model.Laryngoscope Investig Otolaryngol. 2023 Jun 26;8(4):939-945. doi: 10.1002/lio2.1093. eCollection 2023 Aug. Laryngoscope Investig Otolaryngol. 2023. PMID: 37621281 Free PMC article.
References
-
- Reid A, Ha JF. Inhalational injury and the larynx: a review. Burns. 2019;45:1266–1274. - PubMed
-
- Wan J, Zhang G, Qiu Y, Wen C, Fu T. Heat dissipation by blood circulation and airway tissue heat absorption in a canine model of inhalational thermal injury. Burns. 2016;42:548–555. - PubMed
-
- Zhao R, Di LN, Zhao XZ, Wang C, Zhang GA. Measuring surface temperature and grading pathological changes of airway tissue in a canine model of inhalational thermal injury. Burns. 2013;39:767–775. - PubMed
LinkOut - more resources
Full Text Sources