

Haemodynamic left-ventricular changes during dobutamine stress in patients with atrial septal defect assessed with magnetic resonance imaging-based pressure-volume loops
- PMID: 35838181
- PMCID: PMC9796342
- DOI: 10.1111/cpf.12781
Haemodynamic left-ventricular changes during dobutamine stress in patients with atrial septal defect assessed with magnetic resonance imaging-based pressure-volume loops
Abstract
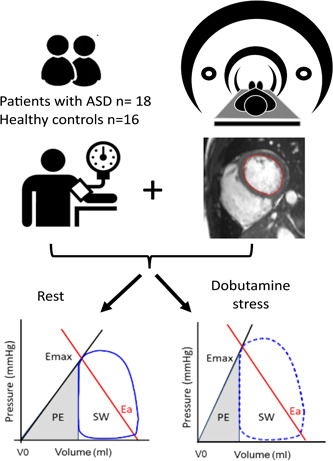
Background: Atrial septal defect (ASD) results in a left-to-right shunt causing right-ventricular (RV) volume overload and decreased cardiac output from the left ventricle. Pressure-volume (PV) loops enable comprehensive assessment of ventricular function and might increase understanding of the pathophysiology of ASD. The aim of this study was to investigate if left-ventricular (LV) haemodynamic response to stress in patients with ASD differs from controls.
Material and methods: Patients with ASD (n = 18, age 51 ± 18) and healthy controls (n = 16, age 35 ± 13) underwent cardiac magnetic resonance (CMR) and brachial cuff pressure measurements at rest and during dobutamine stress. An in-house, validated method was used to compute PV loops.
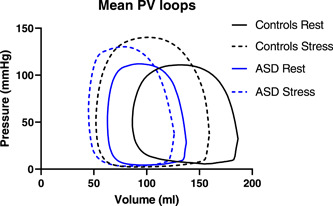
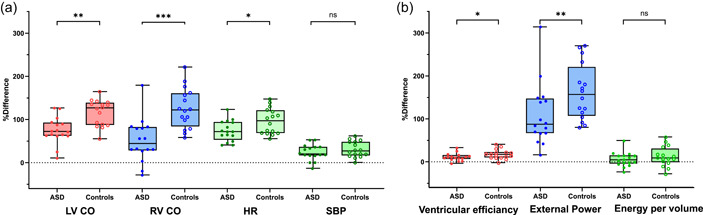
Results: Patients had lower stroke work, potential energy and external power at rest than controls (p < 0.001; p < 0.05; p < 0.05). Stroke work and external power increased and potential energy decreased during stress in patients (p < 0.05; p < 0.0001; p < 0.01) and controls (p < 0.0001; p < 0.001; p < 0.01). Contractility and arterial elastance at rest were higher in patients than controls (p < 0.01; p < 0.01). Contractility increased during stress in both groups (p < 0.0001; p < 0.001). There was no difference between patients and controls in arterio-ventricular coupling.
Conclusion: LV haemodynamic response to stress can be assessed using noninvasive PV loops derived from CMR and brachial blood pressure. Patients with ASD had normal LV energy efficiency, in contrast to other patient groups with decreased cardiac output. Data suggest that patients with ASD had an increased inotropic level at rest with high contractility and heart rate but were able to respond with a further increase during stress, albeit to not as high a cardiac output as controls.
Keywords: atrial septal defect; cardiovascular magnetic imaging; congenital heart defect; heart failure; pressure-volume loops.
© 2022 The Authors. Clinical Physiology and Functional Imaging published by John Wiley & Sons Ltd on behalf of Scandinavian Society of Clinical Physiology and Nuclear Medicine.
Conflict of interest statement
Dr. Heiberg is the founder of Medviso AB, Lund, Sweden, the company that produces the Segment software. The remaining authors declare no conflict of interest.
Figures
Similar articles
-
Alterations in ventricular pumping in patients with atrial septal defect at rest, during dobutamine stress and after defect closure.Clin Physiol Funct Imaging. 2018 Sep;38(5):830-839. doi: 10.1111/cpf.12491. Epub 2017 Dec 13. Clin Physiol Funct Imaging. 2018. PMID: 29235722
-
Atrial septal defect closure in children at young age is beneficial for left ventricular function.Eur Heart J Imaging Methods Pract. 2024 Jun 8;2(1):qyae058. doi: 10.1093/ehjimp/qyae058. eCollection 2024 Jan. Eur Heart J Imaging Methods Pract. 2024. PMID: 39224095 Free PMC article.
-
Patients with volume-loaded right ventricle - quantification of left ventricular hemodynamic response to intervention measured by noninvasive pressure-volume loops.Front Physiol. 2023 Dec 6;14:1291119. doi: 10.3389/fphys.2023.1291119. eCollection 2023. Front Physiol. 2023. PMID: 38124715 Free PMC article.
-
Clinical Applications of Pressure-Volume Assessment in Congenital Heart Disease.J Soc Cardiovasc Angiogr Interv. 2023 Feb 22;2(3):100599. doi: 10.1016/j.jscai.2023.100599. eCollection 2023 May-Jun. J Soc Cardiovasc Angiogr Interv. 2023. PMID: 39130717 Free PMC article. Review.
-
Looking Back, Going Forward: Understanding Cardiac Pathophysiology from Pressure-Volume Loops.Biology (Basel). 2024 Jan 19;13(1):55. doi: 10.3390/biology13010055. Biology (Basel). 2024. PMID: 38275731 Free PMC article. Review.
Cited by
-
Contractility, ventriculoarterial coupling, and stroke work after acute myocardial infarction using CMR-derived pressure-volume loop data.Clin Cardiol. 2024 Jan;47(1):e24216. doi: 10.1002/clc.24216. Clin Cardiol. 2024. PMID: 38269628 Free PMC article.
-
Left Ventricular Diastolic Function in Children with Atrial Septal Defects Improves After Closure by Means of Increased Hydraulic Force.Pediatr Cardiol. 2025 Jun;46(5):1194-1201. doi: 10.1007/s00246-024-03534-5. Epub 2024 Jun 11. Pediatr Cardiol. 2025. PMID: 38861174 Free PMC article.
References
-
- Baumgartner, H. , Bonhoeffer, P. , De Groot, N.M. , De Haan, F. , Deanfield, J.E. , Galie, N. et al. (2010) ESC guidelines for the management of grown‐up congenital heart disease (new version 2010). European Heart Journal, 31, 2915–2957. - PubMed
-
- Brochu, M.C. , Baril, J.F. , Dore, A. , Juneau, M. , De Guise, P. & Mercier, L.A. (2002) Improvement in exercise capacity in asymptomatic and mildly symptomatic adults after atrial septal defect percutaneous closure. Circulation, 106, 1821–1826. Available from: 10.1161/01.CIR.0000029924.90823.E0 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
