

Emerging phenotypes of pulmonary hypertension associated with COPD: a field guide
- PMID: 35838373
- PMCID: PMC9451611
- DOI: 10.1097/MCP.0000000000000890
Emerging phenotypes of pulmonary hypertension associated with COPD: a field guide
Abstract
Purpose of review: Pulmonary hypertension (PH) is a common complication of chronic obstructive lung disease (COPD), but clinical presentation is variable and not always 'proportional' to the severity of the obstructive disease. This review aims to analyze heterogeneity in clinical features of PH-COPD, providing a guide for diagnosis and management according to phenotypes.
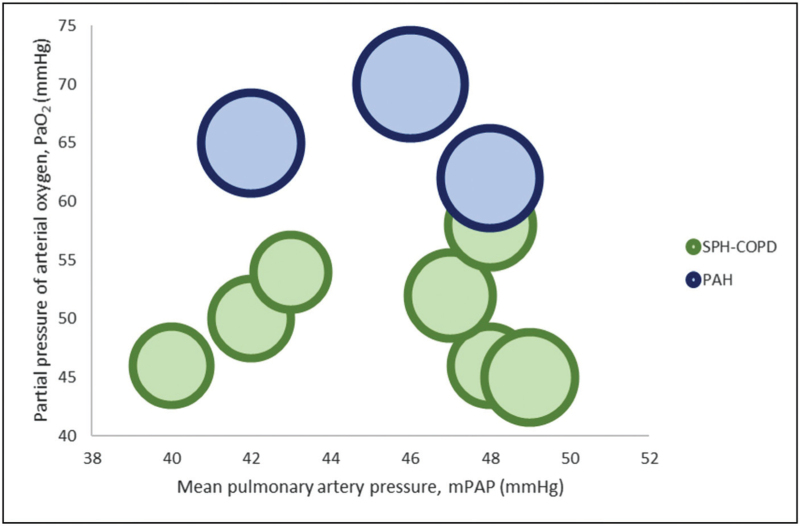
Recent findings: Recent works have focused on severe PH in COPD, providing insights into the characteristics of patients with predominantly vascular disease. The recently recognized 'pulmonary vascular phenotype', characterized by severe PH and mild airflow obstruction with severe hypoxemia, has markedly worse prognosis and may be a candidate for large trials with pulmonary vasodilators. In severe PH, which might be best described by a pulmonary vascular resistance threshold, there may also be a need to distinguish patients with mild COPD (pulmonary vascular phenotype) from those with severe COPD ('Severe COPD-Severe PH' phenotype).
Summary: Correct phenotyping is key to appropriate management of PH associated with COPD. The lack of evidence regarding the use of pulmonary vasodilators in PH-COPD may be due to the existence of previously unrecognized phenotypes with different responses to therapy. This review offers the clinician caring for patients with COPD and PH a phenotype-focused approach to diagnosis and management, aimed at personalized care.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures


References
-
- Kessler R, Faller M, Fourgaut G, et al. . Predictive factors of hospitalization for acute exacerbation in a series of 64 patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1999; 159:158–164. - PubMed
-
- Zeder K, Avian A, Bachmaier G, et al. . Elevated pulmonary vascular resistance predicts mortality in COPD patients. Eur Respir J 2021; 58:2100944. - PubMed
-
This study found PVR >5 WU to be the strongest independent hemodynamic predictor of mortality in COPD patients and may best identify COPD patients with severe pulmonary vascular disease.
-
- Gall H, Felix JF, Schneck FK, et al. . The Giessen Pulmonary Hypertension Registry: Survival in pulmonary hypertension subgroups. J Heart Lung Transplant 2017; 36:957–967. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
