

Association of Access to Crisis Intervention Teams With County Sociodemographic Characteristics and State Medicaid Policies and Its Implications for a New Mental Health Crisis Lifeline
- PMID: 35838666
- PMCID: PMC9287760
- DOI: 10.1001/jamanetworkopen.2022.24803
Association of Access to Crisis Intervention Teams With County Sociodemographic Characteristics and State Medicaid Policies and Its Implications for a New Mental Health Crisis Lifeline
Abstract
Importance: The mental health crisis lifeline 988 will begin operating July 16, 2022. In the absence of appropriately trained first responders, including crisis intervention teams (CITs), persons experiencing behavioral health crises face the risk of incarceration and even death.
Objective: To assess county-level access to CIT in 2015 and 2020 and its association with area characteristics and state policies in 2020.
Design, setting, and participants: This cross-sectional study included 10 430 facilities from the 2015 National Directory of Mental Health Treatment Facilities and 10 591 facilities from the 2020 National Directory of Mental Health Treatment Facilities, attributed to 3142 US counties.
Exposures: Area measures included need (suicide, drug-related overdose mortality), rurality, and demographic characteristics. State-level policies included 5 Medicaid policies enacted prior to 2020 and 2 recent policies intended to assist implementation of the 988 lifeline.
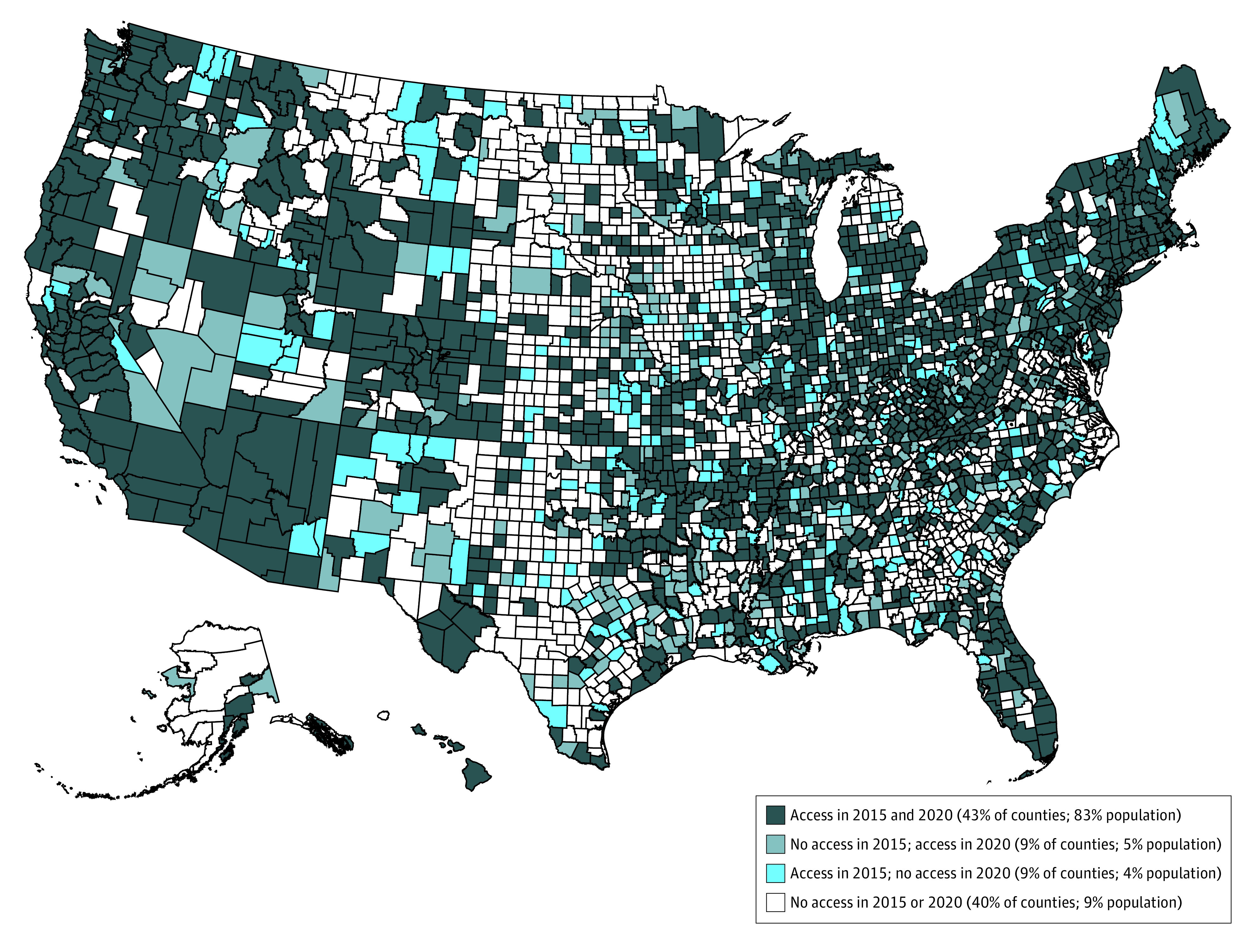
Main outcomes and measures: Whether there was at least 1 facility that reported offering a CIT that handled acute mental health issues at the facility or off-site for each county in 2015 and, separately, in 2020.
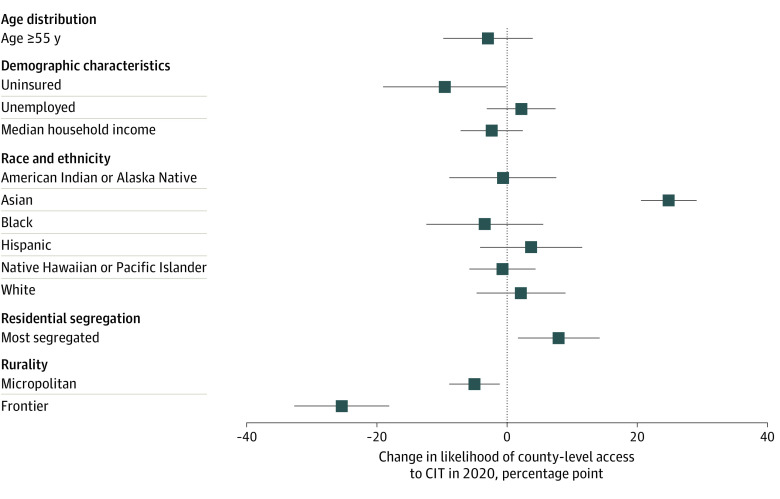
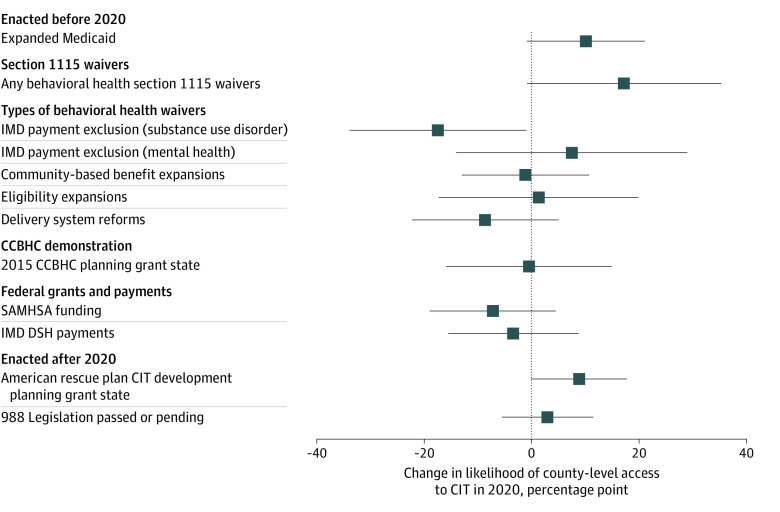
Results: Most US residents (88%) resided in a county with at least 1 facility offering CIT, although half of US counties had no facility offering CIT (2015: 1537 of 3142 [49%]; 2020: 1512 [48%]). Almost 1 in 5 counties, representing 9% of the population, experienced a change in county-level access from 2015 to 2020. Unadjusted analyses indicated residents of counties without vs with CIT access were more likely to be older and uninsured (top quartile of percentage of residents aged >55 years: 502 of 1512 [33%] vs 283 of 1630 [17%]; P < .001; top quartile of percentage of residents uninsured: 500 [33%] vs 285 [17%]; P < .001) and were more likely be rural (frontier: 500 [33%] vs 144 [9%]; P < .001). Similar results, excluding counties in the top quartile of residents aged older than 55 years, were found in adjusted analyses. Counties without vs with CIT access were less likely to be in states that expanded Medicaid (788 [52%] vs 1102 [68%]; P = .01) and in states that allow Medicaid to pay for short-term stays in psychiatric hospitals (34 [2%] vs 73 [4%]; P = .02). Other Medicaid-related associations were not statistically significant in adjusted analyses.
Conclusions and relevance: In this study, most US residents lived in counties with access to at least 1 CIT, but fewer than half of US counties had such access. Policies to encourage facilities in rural counties to offer CIT may help realize the potential of the new lifeline.
Conflict of interest statement
Figures
Comment in
-
Mending the Holes in the Suicide Safety Net.JAMA Netw Open. 2022 Jul 1;5(7):e2225794. doi: 10.1001/jamanetworkopen.2022.25794. JAMA Netw Open. 2022. PMID: 35838676 No abstract available.
Similar articles
-
Race/ethnicity and geographic access to Medicaid substance use disorder treatment facilities in the United States.JAMA Psychiatry. 2014 Feb;71(2):190-6. doi: 10.1001/jamapsychiatry.2013.3575. JAMA Psychiatry. 2014. PMID: 24369387 Free PMC article.
-
Expansion of Telehealth Availability for Mental Health Care After State-Level Policy Changes From 2019 to 2022.JAMA Netw Open. 2023 Jun 1;6(6):e2318045. doi: 10.1001/jamanetworkopen.2023.18045. JAMA Netw Open. 2023. PMID: 37310741 Free PMC article.
-
Geography and the Medicaid mental health care infrastructure: implications for health care reform.JAMA Psychiatry. 2013 Oct;70(10):1084-90. doi: 10.1001/jamapsychiatry.2013.377. JAMA Psychiatry. 2013. PMID: 23965816 Free PMC article.
-
Association of Medicaid Expansion With Opioid Overdose Mortality in the United States.JAMA Netw Open. 2020 Jan 3;3(1):e1919066. doi: 10.1001/jamanetworkopen.2019.19066. JAMA Netw Open. 2020. PMID: 31922561 Free PMC article.
-
Trends in visits to substance use disorder treatment facilities in 2020.J Subst Abuse Treat. 2021 Aug;127:108462. doi: 10.1016/j.jsat.2021.108462. Epub 2021 May 11. J Subst Abuse Treat. 2021. PMID: 34134879 Free PMC article. Review.
Cited by
-
State Policies Associated with Availability of Mobile Crisis Teams.Adm Policy Ment Health. 2025 Jul;52(4):819-827. doi: 10.1007/s10488-024-01368-0. Epub 2024 Mar 18. Adm Policy Ment Health. 2025. PMID: 38498103 Free PMC article.
-
Is access to crisis teams associated with changes in behavioral health mortality?Health Aff Sch. 2025 Jan 15;3(1):qxaf003. doi: 10.1093/haschl/qxaf003. eCollection 2025 Jan. Health Aff Sch. 2025. PMID: 39877431 Free PMC article.
-
What Explains Changes in Availability of Specialty Mental Health Services in Organized Settings?Milbank Q. 2022 Dec;100(4):1166-1191. doi: 10.1111/1468-0009.12592. Epub 2022 Dec 28. Milbank Q. 2022. PMID: 36575952 Free PMC article.
-
Changes in Specialty Crisis Services Offered Before and After the Launch of the 988 Suicide and Crisis Lifeline.JAMA Psychiatry. 2025 Apr 1;82(4):379-385. doi: 10.1001/jamapsychiatry.2024.4548. JAMA Psychiatry. 2025. PMID: 39878975
-
Market Factors Associated with Comprehensive Behavioral Health Crisis Care Availability: A Resource Dependence Theory Study.Inquiry. 2024 Jan-Dec;61:469580241256822. doi: 10.1177/00469580241256822. Inquiry. 2024. PMID: 38842194 Free PMC article.
References
-
- Ahmad F, Rossen L, Sutton P. Vital Statistics Rapid Release: provisional drug overdose death counts. Accessed March 16, 2022. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
-
- Hedegaard H, Curtin SC, Warner M. Increase in suicide mortality in the United States, 1999-2018. April 2020. Accessed July 6, 2021. https://stacks.cdc.gov/view/cdc/86670 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
