

Evaluating the rare cases of cortical vertigo using disconnectome mapping
- PMID: 35838791
- PMCID: PMC9653368
- DOI: 10.1007/s00429-022-02530-w
Evaluating the rare cases of cortical vertigo using disconnectome mapping
Abstract
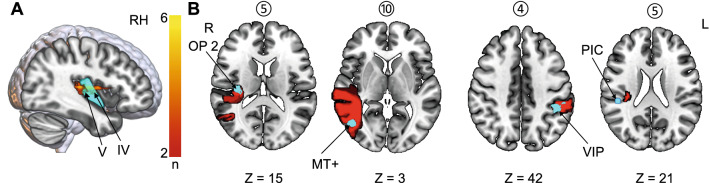
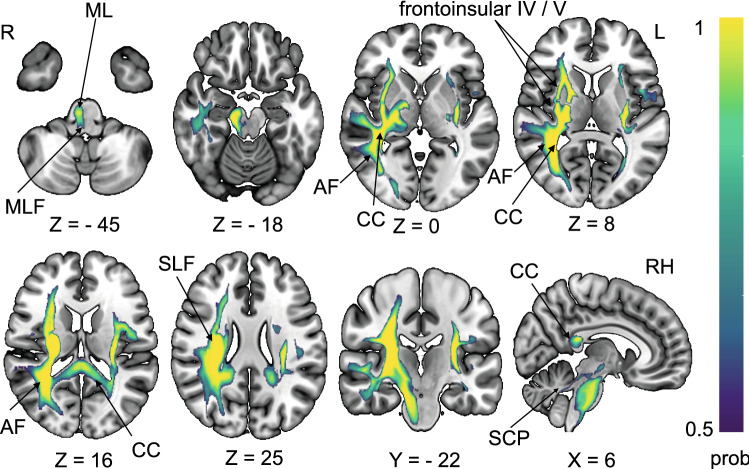
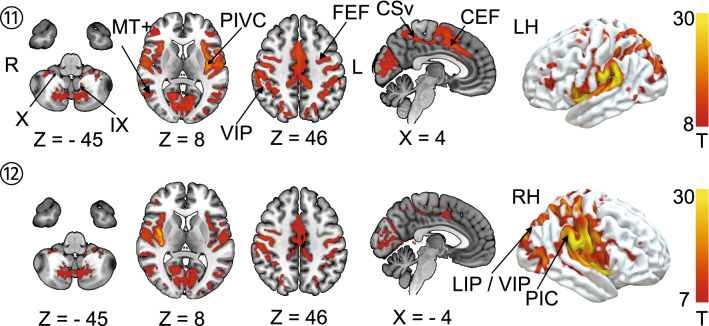
In rare cases, cortical infarcts lead to vertigo. We evaluated structural and functional disconnection in patients with acute vertigo due to unilateral ischemic cortical infarcts compared to infarcts without vertigo in a similar location with a focus on the connectivity of the vestibular cortex, i.e., the parieto-opercular (retro-)insular cortex (PIVC). Using lesion maps from the ten published case reports, we computed lesion-functional connectivity networks in a set of healthy individuals from the human connectome project. The probability of lesion disconnection was evaluated by white matter disconnectome mapping. In all ten cases with rotational vertigo, disconnections of interhemispheric connections via the corpus callosum were present but were spared in lesions of the PIVC without vertigo. Further, the arcuate fascicle was affected in 90% of the lesions that led to vertigo and spared in lesions that did not lead to vertigo. The lesion-functional connectivity network included vestibulo-cerebellar hubs, the vestibular nuclei, the PIVC, the retro-insular and posterior insular cortex, the multisensory vestibular ventral intraparietal area, motion-sensitive areas (temporal area MT+ and cingulate visual sulcus) as well as hubs for ocular motor control (lateral intraparietal area, cingulate and frontal eye fields). However, this was not sufficient to differentiate between lesions with and without vertigo. Disruption of interhemispheric connections of both PIVC via the corpus callosum and intra-hemispheric disconnection via the arcuate fascicle might be the distinguishing factor between vestibular cortical network lesions that manifest with vertigo compared to those without vertigo.
Keywords: Corpus callosum; Cortical vertigo; Disconnectome; Insula; PIVC; Vestibular.
© 2022. The Author(s).
Conflict of interest statement
The authors have not disclosed any competing interests.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
