

Cross-sectional comparison of age- and gender-related comorbidities in people living with HIV in Canada
- PMID: 35839056
- PMCID: PMC11132354
- DOI: 10.1097/MD.0000000000029850
Cross-sectional comparison of age- and gender-related comorbidities in people living with HIV in Canada
Abstract
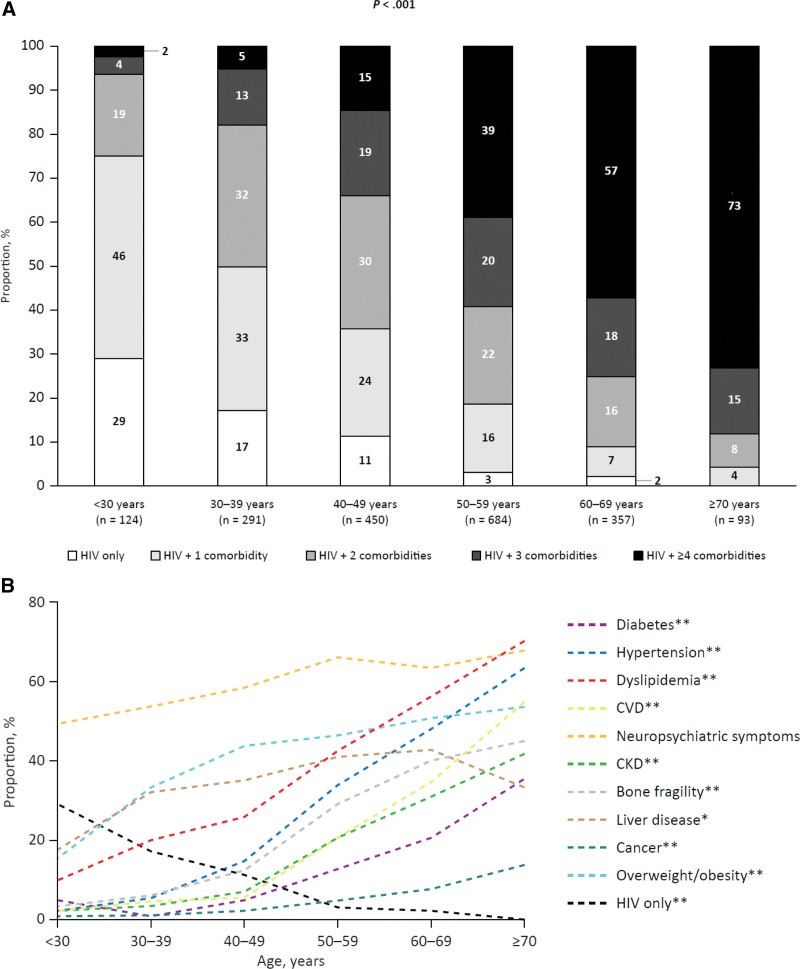
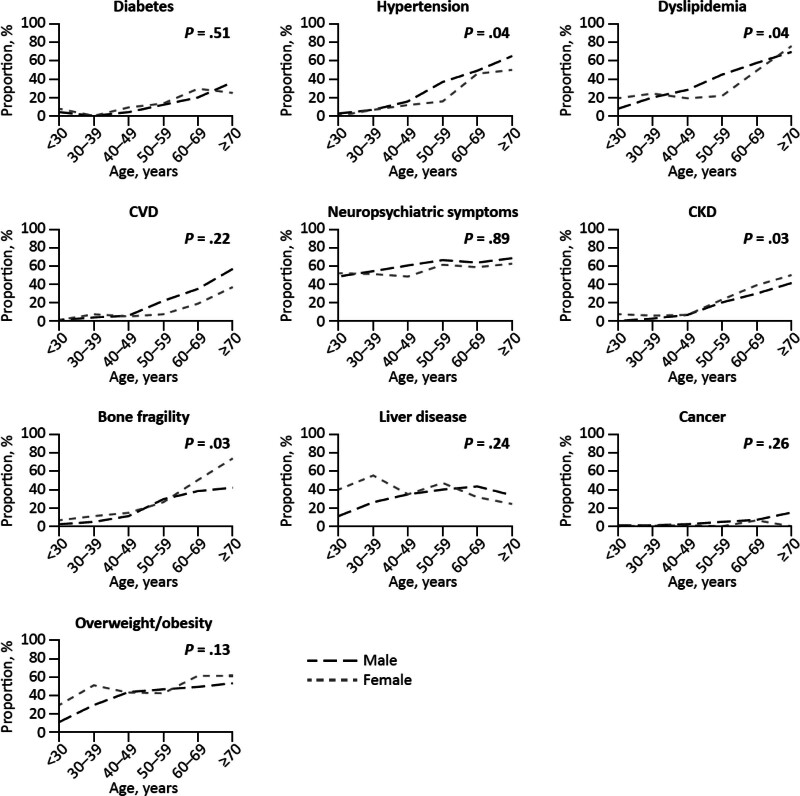
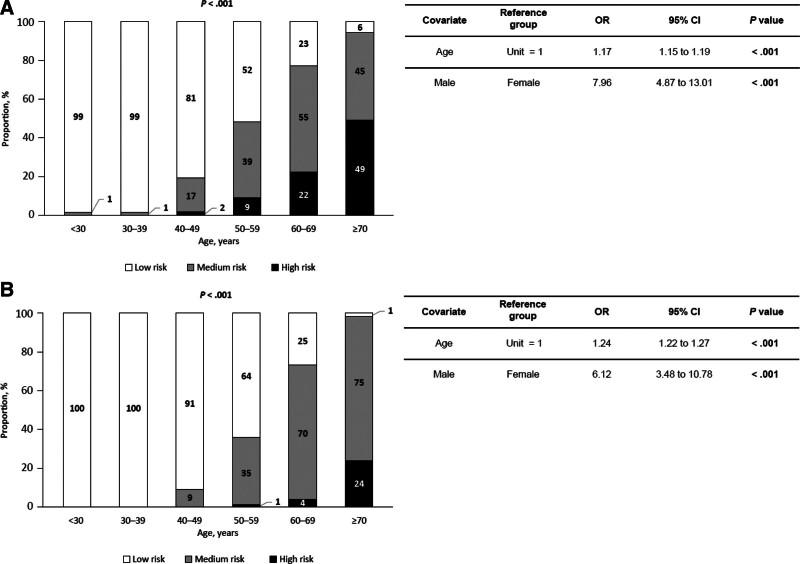
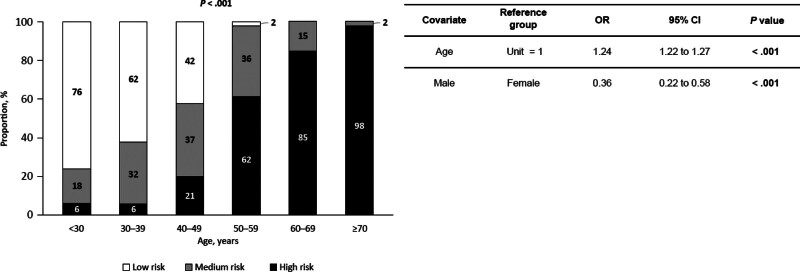
Because antiretroviral therapy (ART) is allowing people living with human immunodeficiency virus (PLWH) to survive longer, they are developing more age-related comorbidities. We evaluated the effects of age and gender on the burden of age-related comorbidities among PLWH. In this retrospective real-world study, de-identified data were extracted from the medical charts of 2000 HIV-positive adults on ART across 10 sites in Canada. The prevalence of age-related comorbidities was determined in 6 age subgroups (<30, 30-39, 40-49, 50-59, 60-69, and ≥70 years). The effects of gender on these comorbidities were also examined. Risks of cardiovascular disease and chronic kidney disease (CKD) were calculated using the Framingham and D:A:D equations. Most persons were White (68%), male (87%), and virologically suppressed (94%). The mean age was 50.3 years (57% aged ≥50 years), and mean CD4+ T-cell count was 616 cells/mm3. The most common comorbidities were neuropsychiatric symptoms (61%), overweight/obesity (43%), liver disease (37%), and dyslipidemia (37%). The mean number of comorbidities increased across age subgroups (P < .001). Across all age subgroups, the prevalence of hypertension (P = .04), dyslipidemia (P = .04), CKD (P = .03), bone fragility (P = .03), and depression (P = .02) differed between males and females. Both age (P < .001) and gender (P < .001) impacted cardiovascular disease and CKD risk. Age and gender influenced the burden, types, and risks of age-related comorbidities in PLWH in this Canadian cohort. These comorbidities should be diagnosed and treated in routine clinical practice.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
J.M.B. received conference sponsorship from Gilead Sciences and ViiV Healthcare; consultancy fees from Gilead Sciences, ViiV Healthcare, and Merck; and speaker fees from Gilead Sciences. J.-G.B. reports grants to his institution from ViiV Healthcare, Gilead Sciences, and Merck and honoraria for consultancy, ad-boards, or conferences from ViiV Healthcare, Gilead Sciences, and Merck. J.J.d.W. served on advisory boards and as a speaker for ViiV Healthcare and Gilead Sciences. C.F. received funds for the development of hepatitis C virus learning modules for iCare Education Inc. (paid to Dr. Fraser) and funding for educational conferences, continuing medical education presentations, and clinical trials from AbbVie, Gilead Sciences, Merck, and ViiV Healthcare (paid to institution). G.R. is member of medical advisory boards for Gilead Sciences, Moderna, ViiV Healthcare, and Merck. R.T. received honoraria from Gilead Sciences for presentations, consultations, and advisory boards. His institution receives funding from Gilead Sciences for its HIV and preexposure prophylaxis databases and for intervention projects. K.L. received advisory board fees from ViiV Healthcare and Gilead Sciences. M.S. received consultation fees on advisory boards for Gilead Sciences and Merck. J.P. supplied data collection and management services, which were funded by Gilead Sciences Canada. R.-P.L. is an employee of Gilead Sciences Canada. H.T. is a former employee of Gilead Sciences Canada. K.J.K. is an employee of Gilead Sciences, Inc. and a former employee of Gilead Sciences Canada. A.W. received consulting fees and honoraria from Merck, Gilead Sciences, and ViiV Healthcare; received funding for regional and provincial programming from Merck, Gilead Sciences, and ViiV Healthcare; and currently participates in clinical trials for Merck, Gilead Sciences, and ViiV Healthcare. H.L. and H.J. have no conflicts of interest to disclose.
Figures
Similar articles
-
Excess burden of age-associated comorbidities among people living with HIV in British Columbia, Canada: a population-based cohort study.BMJ Open. 2021 Jan 8;11(1):e041734. doi: 10.1136/bmjopen-2020-041734. BMJ Open. 2021. PMID: 33419911 Free PMC article.
-
Evolution of comorbidities in people living with HIV between 2004 and 2014: cross-sectional analyses from ANRS CO3 Aquitaine cohort.BMC Infect Dis. 2020 Nov 16;20(1):850. doi: 10.1186/s12879-020-05593-4. BMC Infect Dis. 2020. PMID: 33198667 Free PMC article.
-
Incidence of select chronic comorbidities among a population-based cohort of HIV-positive individuals receiving highly active antiretroviral therapy.Curr Med Res Opin. 2019 Nov;35(11):1955-1963. doi: 10.1080/03007995.2019.1645999. Epub 2019 Aug 26. Curr Med Res Opin. 2019. PMID: 31315470
-
Chronic Kidney Disease in Persons Living with HIV: A Systematic Review.J Assoc Nurses AIDS Care. 2018 Sep-Oct;29(5):655-666. doi: 10.1016/j.jana.2018.04.004. Epub 2018 Apr 19. J Assoc Nurses AIDS Care. 2018. PMID: 29751988
-
Cardiac and Renal Comorbidities in Aging People Living With HIV.Circ Res. 2024 May 24;134(11):1636-1660. doi: 10.1161/CIRCRESAHA.124.323948. Epub 2024 May 23. Circ Res. 2024. PMID: 38781295 Free PMC article. Review.
Cited by
-
Reporting and handling of missing data in published studies of co-morbid hypertension and diabetes among people living with HIV/AIDS: a systematic review.BMC Med Res Methodol. 2025 Jul 30;25(1):180. doi: 10.1186/s12874-025-02630-1. BMC Med Res Methodol. 2025. PMID: 40739213 Free PMC article.
-
Comorbidities in people living with HIV/AIDS and their impact on outpatient dental care.Braz Oral Res. 2025 Apr 4;39:e035. doi: 10.1590/1807-3107bor-2025.vol39.035. eCollection 2025. Braz Oral Res. 2025. PMID: 40197929 Free PMC article.
-
Role of the pharmacist caring for people at risk of or living with HIV in Canada.Can Pharm J (Ott). 2024 Aug 2;157(5):218-239. doi: 10.1177/17151635241267350. eCollection 2024 Sep-Oct. Can Pharm J (Ott). 2024. PMID: 39310805 Free PMC article. No abstract available.
References
-
- Public Health Agency of Canada. Estimates of HIV incidence, prevalence and Canada’s progress on meeting the 90-90-90 HIV targets, 2018. December 2020. Available at: https://www.canada.ca/en/public-health/services/publications/diseases-co... [access date January 12, 2022].
-
- Marcus JL, Leyden W, Anderson AN, et al. . Combination antiretroviral therapy (ART) has dramatically improved life expectancy for people with HIV (PWH), but recent data comparing overall lifespan and comorbidity-free years by HIV status are lacking. Presented at: 2020 Conference on Retroviruses and Opportunistic Infections; March 8–11, 2020; Boston, USA; virtual.
-
- The World Bank. Life expectancy at birth, total (years)—Canada. Available at: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=CA [access date January 12, 2022].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
