

Effect of exercise training after bariatric surgery: A 5-year follow-up study of a randomized controlled trial
- PMID: 35839214
- PMCID: PMC9286216
- DOI: 10.1371/journal.pone.0271561
Effect of exercise training after bariatric surgery: A 5-year follow-up study of a randomized controlled trial
Abstract
Background and objectives: We previously showed in a 6-month randomized controlled trial that resistance training and protein supplementation after bariatric surgery (Roux-en-Y gastric bypass, RYGB) improved muscle strength without significant effect on weight loss and body composition changes. We performed a 5-year follow-up study in these subjects with the aim 1) to assess the long-term effect of this exercise training intervention and 2) to analyze associations between habitual physical activity (PA) and weight regain at 5 years.
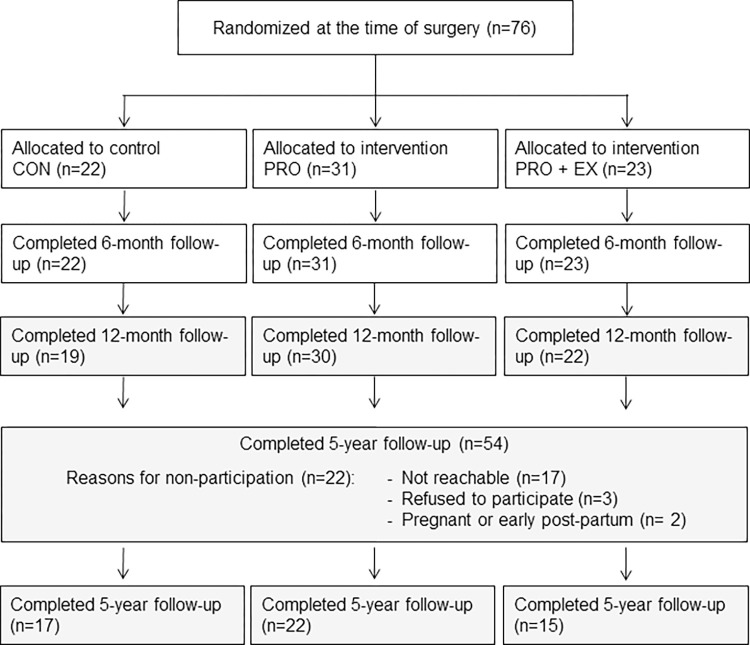
Methods: Fifty-four out of 76 initial participants (follow-up rate of 71%) completed the 5-year follow-up examination (controls, n = 17; protein supplementation, n = 22; protein supplementation and resistance training, n = 15). We measured body weight and composition (DXA), lower-limb strength (leg-press one-repetition maximum) and habitual PA (Actigraph accelerometers and self-report). Weight regain at 5 years was considered low when <10% of 12-month weight loss.
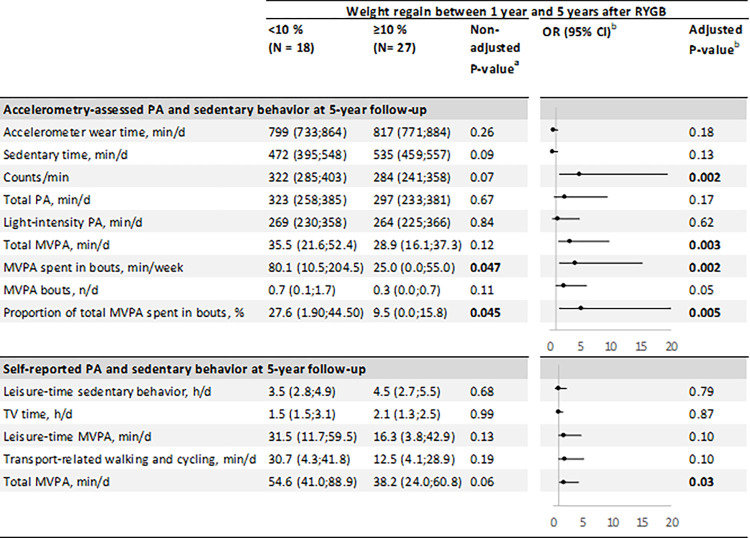
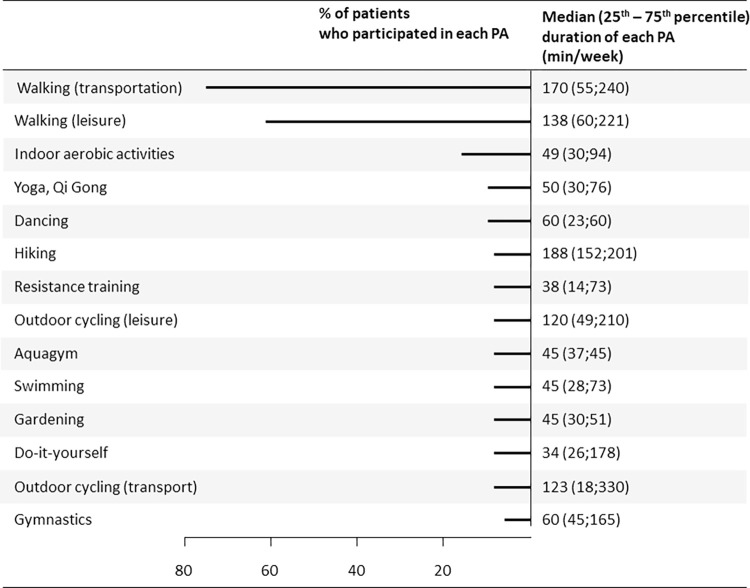
Results: Mean (SD) time elapse since RYGB was 5.7 (0.9) y. At 5 years, weight loss was 32.8 (10.1) kg, with a mean weight regain of 5.4 (SD 5.9) kg compared with the 12-month assessment. Moderate-to-vigorous PA (MVPA) assessed by accelerometry did not change significantly compared with pre-surgery values (+5.2 [SD 21.7] min/d, P = 0.059), and only 4 (8.2%) patients reported participation in resistance training. Muscle strength decreased over time (overall mean [SD]: -49.9 [53.5] kg, respectively, P<0.001), with no statistically significant difference between exercise training intervention groups. An interquartile increase in MVPA levels was positively associated with lower weight regain (OR [95% CI]: 3.27 [1.41;9.86]).
Conclusions: Early postoperative participation in a resistance training protocol after bariatric surgery was not associated with improved muscle strength after 5 years of follow-up; however, increasing physical activity of at least moderate intensity may promote weight maintenance after surgery. PA may therefore play an important role in the long-term management of patients with obesity after undergoing bariatric procedure.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief. 2020; 1–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
