

Prophylactic furosemide to prevent transfusion-associated circulatory overload: a randomized controlled study in rats
- PMID: 35840620
- PMCID: PMC9287390
- DOI: 10.1038/s41598-022-16465-z
Prophylactic furosemide to prevent transfusion-associated circulatory overload: a randomized controlled study in rats
Abstract
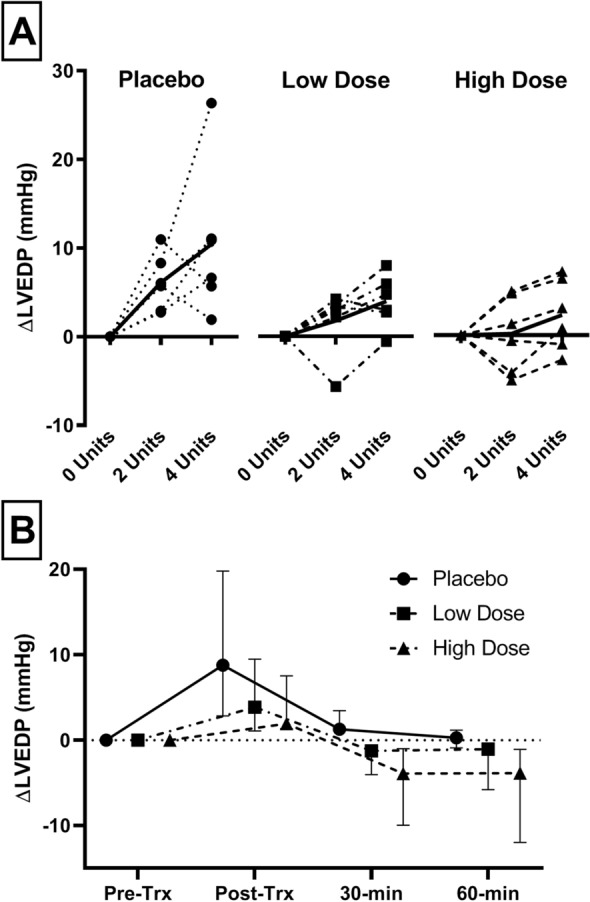
Transfusion-associated circulatory overload (TACO) is the leading cause of transfusion related morbidity and mortality. The only treatment is empirical use of furosemide. Our aim was to investigate if furosemide can prevent TACO. A randomized controlled trial was performed using a previously validated two-hit rat model for TACO. Volume incompliance was induced (first hit) in anemic, anesthetized Lewis rats. Rats were randomized to placebo, low-dose (5 mg kg-1) or high-dose (15 mg kg-1) furosemide-administered prior to transfusion (second-hit) and divided over two doses. Primary outcome was change in left-ventricular end-diastolic pressure (∆LVEDP) pre- compared to post-transfusion. Secondary outcomes included changes in preload, afterload, contractility and systemic vascular resistance, as well as pulmonary outcomes. Furosemide treated animals had a significantly lower ∆LVEDP compared to placebo (p = 0.041), a dose-response effect was observed. ∆LVEDP in placebo was median + 8.7 mmHg (IQR 5.9-11), + 3.9 (2.8-5.6) in the low-dose and 1.9 (- 0.6 to 5.6) in the high-dose group. The effect of furosemide became apparent after 15 min. While urine output was significantly higher in furosemide treated animals (p = 0.03), there were no significant changes in preload, afterload, contractility or systemic vascular resistance. Furosemide rapidly and dose-dependently decreases the rise in hydrostatic pulmonary pressure following transfusion, essential for preventing TACO.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Blumberg N, et al. An association between decreased cardiopulmonary complications (transfusion-related acute lung injury and transfusion-associated circulatory overload) and implementation of universal leukoreduction of blood transfusions. Transfusion. 2010;50(12):2738–2744. doi: 10.1111/j.1537-2995.2010.02748.x. - DOI - PMC - PubMed
-
- Andrzejewski C, Jr, et al. Hemotherapy bedside biovigilance involving vital sign values and characteristics of patients with suspected transfusion reactions associated with fluid challenges: Can some cases of transfusion-associated circulatory overload have proinflammatory aspects? Transfusion. 2012;52(11):2310–2320. doi: 10.1111/j.1537-2995.2012.03595.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
