

Cut-off values for diagnosis of G6PD deficiency by flow cytometry in Thai population
- PMID: 35840819
- PMCID: PMC9463333
- DOI: 10.1007/s00277-022-04923-7
Cut-off values for diagnosis of G6PD deficiency by flow cytometry in Thai population
Abstract
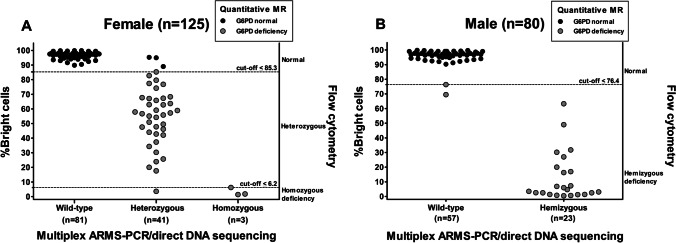
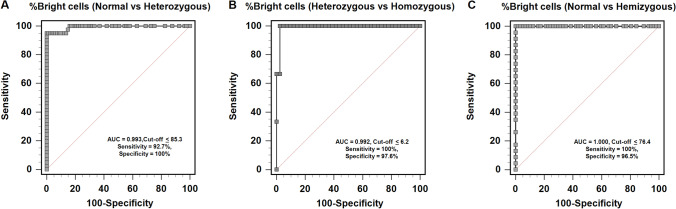
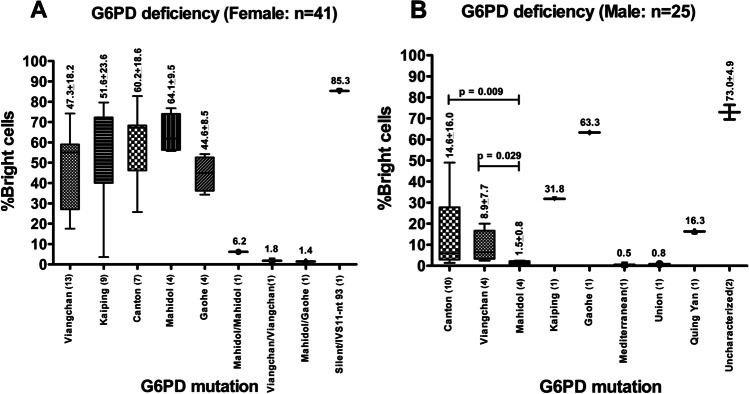
In heterozygous females, X-inactivation causes a change in glucose-6-phosphate dehydrogenase (G6PD) activity from normal to deficient. Most G6PD screening tests are used to accurately diagnose hemizygous males, but they are less reliable for diagnosing heterozygous females. This study established flow cytometric cut-off values for screening of G6PD deficiency in hemizygous males and heterozygous or homozygous females. We studied 205 (125 females, 80 males) leftover blood samples from quantitative methemoglobin reduction (MR) screening. G6PD gene mutations determined by multiplex amplification refractory mutation system-polymerase chain reaction and direct DNA sequencing were used as the gold standard reference. Accuracy of the test, including the sensitivity, specificity, and positive and negative predictive values, was analyzed using MedCalc software. The optimal cut-off values for classification of %red blood cells with normal G6PD activity or %bright cells into homozygous normal, heterozygous, and homozygous deficiency in females were 85.4-100%, 6.3-85.3%, and 0-6.2%, respectively (sensitivity 93.2%, specificity 100%). The cut-offs for classification into hemizygous normal and hemizygous deficiency in males were 76.5-100% and 0-76.4%, respectively (sensitivity 100%, specificity 96.5%). Flow cytometry can be used to differentiate heterozygous females with intermediate phenotype from homozygous females, but cannot distinguish between heterozygous females with extreme phenotype and homozygous females. By flow cytometry, heterozygous and homozygous deficiency was detected in 29.6% and 3.2% of females, respectively. Among males, hemizygous deficiency was found in 31.3%. Flow cytometry can be used to screen patients with G6PD deficiency, and reliably and efficiently identify heterozygous and homozygous females, and hemizygous males based on cellular G6PD activity.
Keywords: Bright cells; G6PD mutation; Intracellular G6PD activity; Multiplex amplification refractory mutation system-polymerase chain reaction (multiplex ARMS-PCR); Quantitative MR; Thai.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Cytochemical flow analysis of intracellular G6PD and aggregate analysis of mosaic G6PD expression.Eur J Haematol. 2018 Mar;100(3):294-303. doi: 10.1111/ejh.13013. Epub 2018 Jan 15. Eur J Haematol. 2018. PMID: 29240263 Free PMC article.
-
Evaluation of a flow cytometric test for G6PD-deficient erythrocytes.Trop Med Int Health. 2021 Apr;26(4):462-468. doi: 10.1111/tmi.13547. Epub 2021 Feb 2. Trop Med Int Health. 2021. PMID: 33415798
-
Glucose-6-phosphate dehydrogenase deficiency detection using fluorocytometric assay: Evaluation after 1 year of clinical implementation.Cytometry B Clin Cytom. 2025 Mar;108(2):161-171. doi: 10.1002/cyto.b.22207. Epub 2024 Oct 2. Cytometry B Clin Cytom. 2025. PMID: 39354868
-
Glucose-6-phosphate dehydrogenase deficiency and malaria: cytochemical detection of heterozygous G6PD deficiency in women.J Histochem Cytochem. 2009 Nov;57(11):1003-11. doi: 10.1369/jhc.2009.953828. Epub 2009 Jun 22. J Histochem Cytochem. 2009. PMID: 19546473 Free PMC article. Review.
-
Glucose-6-phosphate dehydrogenase laboratory assay: How, when, and why?IUBMB Life. 2009 Jan;61(1):27-34. doi: 10.1002/iub.137. IUBMB Life. 2009. PMID: 18942156 Review.
Cited by
-
A Review of the Current Status of G6PD Deficiency Testing to Guide Radical Cure Treatment for Vivax Malaria.Pathogens. 2023 Apr 27;12(5):650. doi: 10.3390/pathogens12050650. Pathogens. 2023. PMID: 37242320 Free PMC article. Review.
-
Molecular characterization of G6PD mutations identifies new mutations and a high frequency of intronic variants in Thai females.PLoS One. 2023 Nov 15;18(11):e0294200. doi: 10.1371/journal.pone.0294200. eCollection 2023. PLoS One. 2023. PMID: 37967096 Free PMC article.
-
Genetic analysis and molecular basis of G6PD deficiency among malaria patients in Thailand: implications for safe use of 8-aminoquinolines.Malar J. 2024 Feb 2;23(1):38. doi: 10.1186/s12936-024-04864-8. Malar J. 2024. PMID: 38308253 Free PMC article.
-
Improved genetic screening with zygosity detection through multiplex high-resolution melting curve analysis and biochemical characterisation for G6PD deficiency.Trop Med Int Health. 2025 May;30(5):437-457. doi: 10.1111/tmi.14105. Epub 2025 Mar 13. Trop Med Int Health. 2025. PMID: 40078033 Free PMC article.
References
-
- Charoenkwan P, Tantiprabha W, Sirichotiyakul S, Phusua A, Sanguansermsri T. Prevalence and molecular characterization of glucose-6-phosphate dehydrogenase deficiency in northern Thailand. Southeast Asian J Trop Med Public Health. 2014;45(1):187–193. - PubMed
-
- Phompradit P, Kuesap J, Chaijaroenkul W, Rueangweerayut R, Hongkaew Y, Yamnuan R, Na-Bangchang K. Prevalence and distribution of glucose-6-phosphate dehydrogenase (G6PD) variants in Thai and Burmese populations in malaria endemic areas of Thailand. Malar J. 2011;10:368. doi: 10.1186/1475-2875-10-368. - DOI - PMC - PubMed
-
- World Health Organization . Testing for G6PD deficiency for safe use of primaquine in radical cure of P.vivax and P.ovale: Policy brief. Geneva, Switzerland: World Health Organization; 2016.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
