

Comparison of region-of-interest delineation methods for diffusion tensor imaging in patients with cervical spondylotic radiculopathy
- PMID: 35840941
- PMCID: PMC9284815
- DOI: 10.1186/s12891-022-05639-5
Comparison of region-of-interest delineation methods for diffusion tensor imaging in patients with cervical spondylotic radiculopathy
Abstract
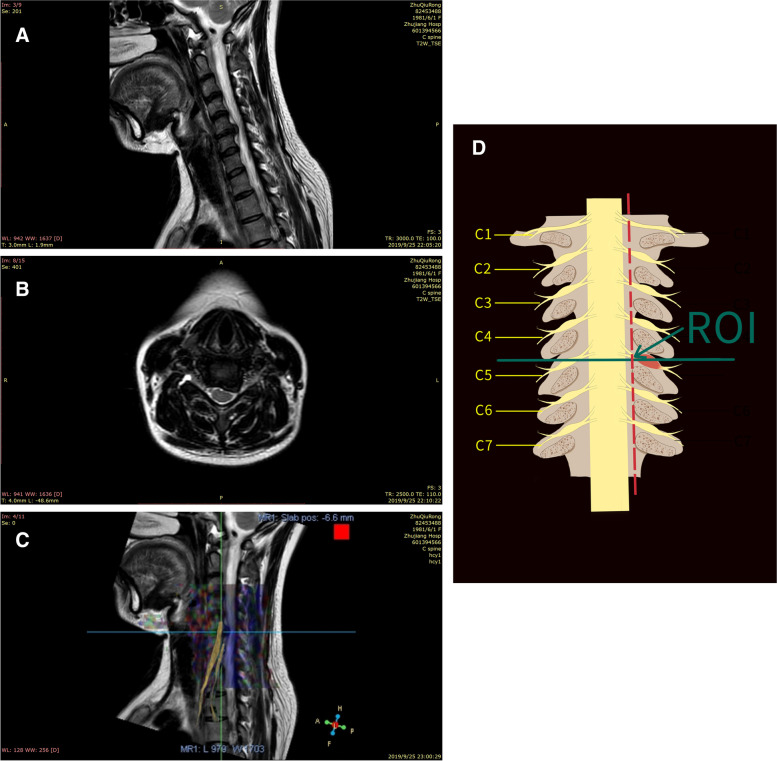
Background: Diffusion tensor imaging is a promising technique for determining the responsible lesion of cervical radiculopathy, but the selection and delineation of the region of interest (ROI) affect the results. This study explored the impact of different ROI sketching methods on the repeatability and consistency of DTI measurement values in patients with cervical spondylotic radiculopathy (CSR).
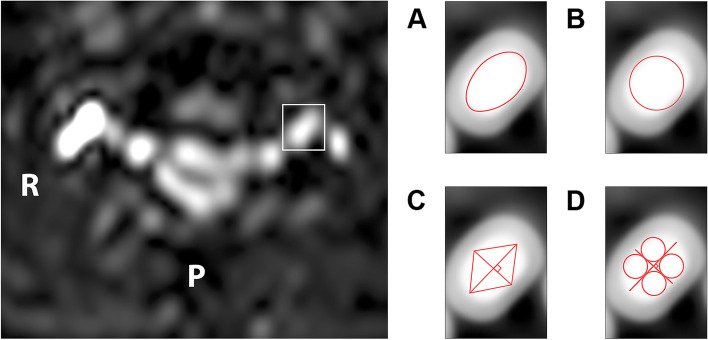
Methods: This retrospective study included CSR patients who underwent DTI imaging. The images were analyzed independently by two radiologists. Four delineation methods were used: freehand method, maximum roundness, quadrilateral method, and multi-point averaging method. They re-examined the images 6 weeks later. The intra-class correlation coefficient (ICC) was used to investigate the consistency between the two measurements and the reproducibility between two radiologists.
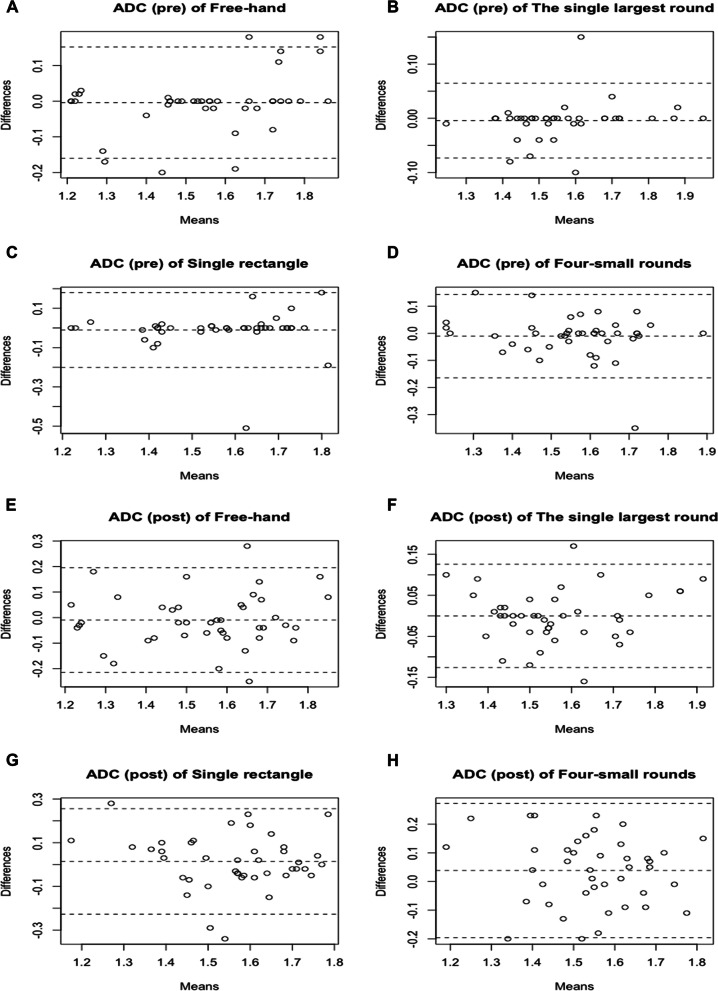
Results: Forty-two CSR patients were included in this study. The distribution of the compressed nerve roots was five C4, eight C5, sixteen C6, eleven C7, and two C8. No differences were found among the four methods in fractional anisotropy (FA) or apparent diffusion coefficient (ADC), irrespective of radiologists (all P>0.05). Similar results were observed between the first and second measurements (all P>0.05), but some significant differences were observed for radiologist 2 for the four-small rounds method (P=0.033). The freehand and single largest circle methods were the two methods with the highest ICC between the two measurements and the two radiologists (all ICC >0.90).
Conclusion: The freehand and single largest circle methods were the most consistent methods for delineating DTI ROI in patients with CSR.
Keywords: Cervical radiculopathy; Diffusion tensor imaging; Imaging parameters.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Childress MA, Becker BA. Nonoperative Management of Cervical Radiculopathy. Am Fam Physician. 2016;93:746–754. - PubMed
-
- Bono CM, Ghiselli G, Gilbert TJ, Kreiner DS, Reitman C, Summers JT, Baisden JL, Easa J, Fernand R, Lamer T, et al. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011;11:64–72. doi: 10.1016/j.spinee.2010.10.023. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
