

Progressive loss of hearing and balance in superficial siderosis due to occult spinal dural defects
- PMID: 35841407
- PMCID: PMC9849153
- DOI: 10.1007/s00405-022-07523-3
Progressive loss of hearing and balance in superficial siderosis due to occult spinal dural defects
Abstract
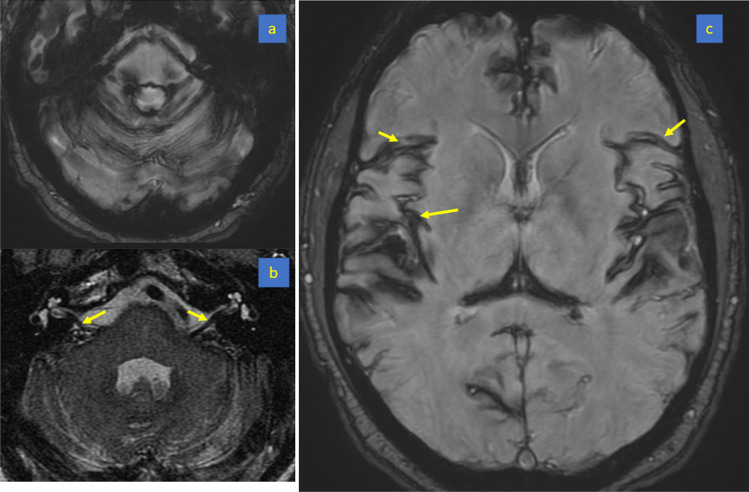
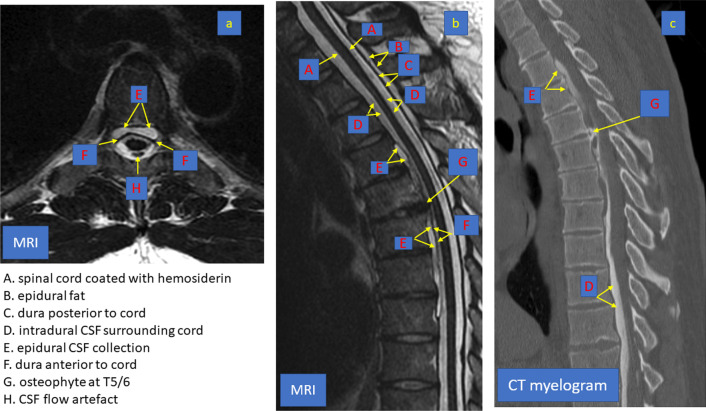
Purpose: Superficial siderosis, a progressive, debilitating, neurological disease, often presents with bilateral impairment of auditory and vestibular function. We highlight that superficial siderosis is often due to a repairable spinal dural defect of the type that can also cause spontaneous intracranial hypotension.
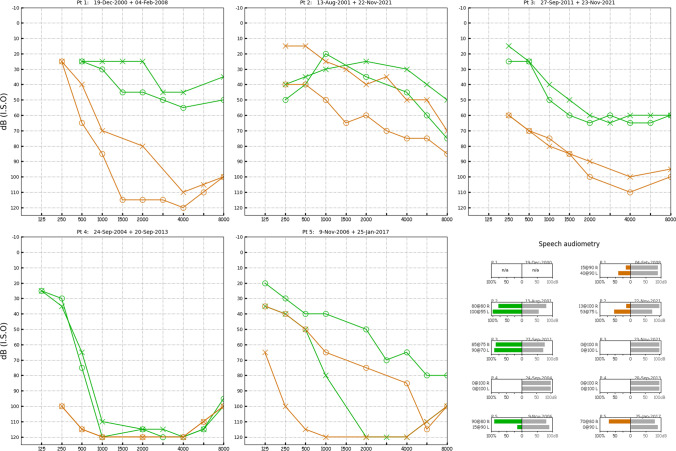
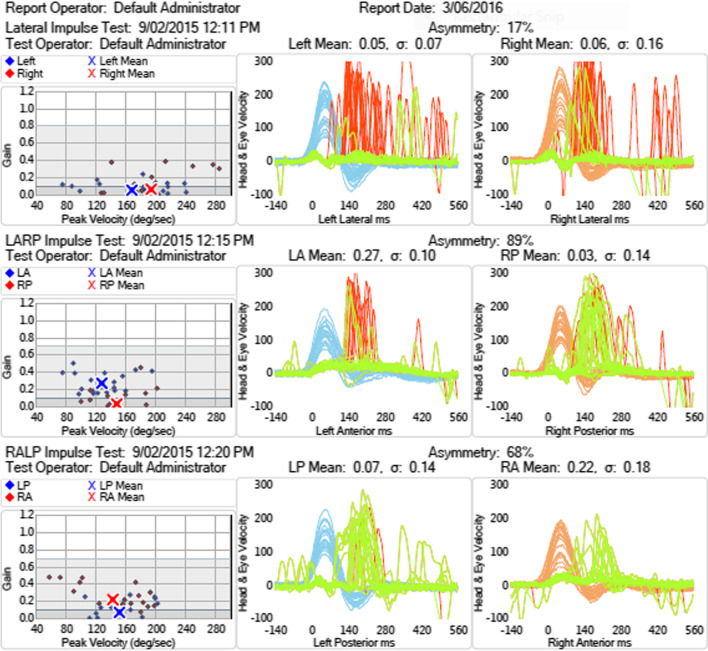
Methods: Retrospective chart review of five patients presenting with moderate to severe, progressive bilateral sensorineural hearing loss as well as vestibular loss. All patients had developed superficial siderosis from spinal dural defects: three after trauma, one after spinal surgery and one from a thoracic discogenic microspur.
Results: The diagnosis was made late in all five patients; despite surgical repair in four, hearing and vestibular loss failed to improve.
Conclusions: In patients presenting with progressive bilateral sensorineural hearing loss, superficial siderosis should be considered as a possible cause. If these patients also have bilateral vestibular loss, cerebellar impairment and anosmia, then the diagnosis is likely and the inevitable disease progress might be halted by finding and repairing the spinal dural defect.
Keywords: CSF leak; Deafness; Spinal dural defects; Superficial siderosis; Vestibulopathy.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest or any financial interests to declare.
Figures
References
-
- Pribitkin EA, Rondinella L, Rosenberg SI, Yousem DM. Superficial siderosis of the central nervous system: an underdiagnosed cause of sensorineural hearing loss and ataxia. Am J Otol. 1994;15(3):415–418. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
