

Cognitive-motor dissociation and time to functional recovery in patients with acute brain injury in the USA: a prospective observational cohort study
- PMID: 35841909
- PMCID: PMC9476646
- DOI: 10.1016/S1474-4422(22)00212-5
Cognitive-motor dissociation and time to functional recovery in patients with acute brain injury in the USA: a prospective observational cohort study
Abstract
Background: Recovery trajectories of clinically unresponsive patients with acute brain injury are largely uncertain. Brain activation in the absence of a behavioural response to spoken motor commands can be detected by EEG, also known as cognitive-motor dissociation. We aimed to explore the role of cognitive-motor dissociation in predicting time to recovery in patients with acute brain injury.
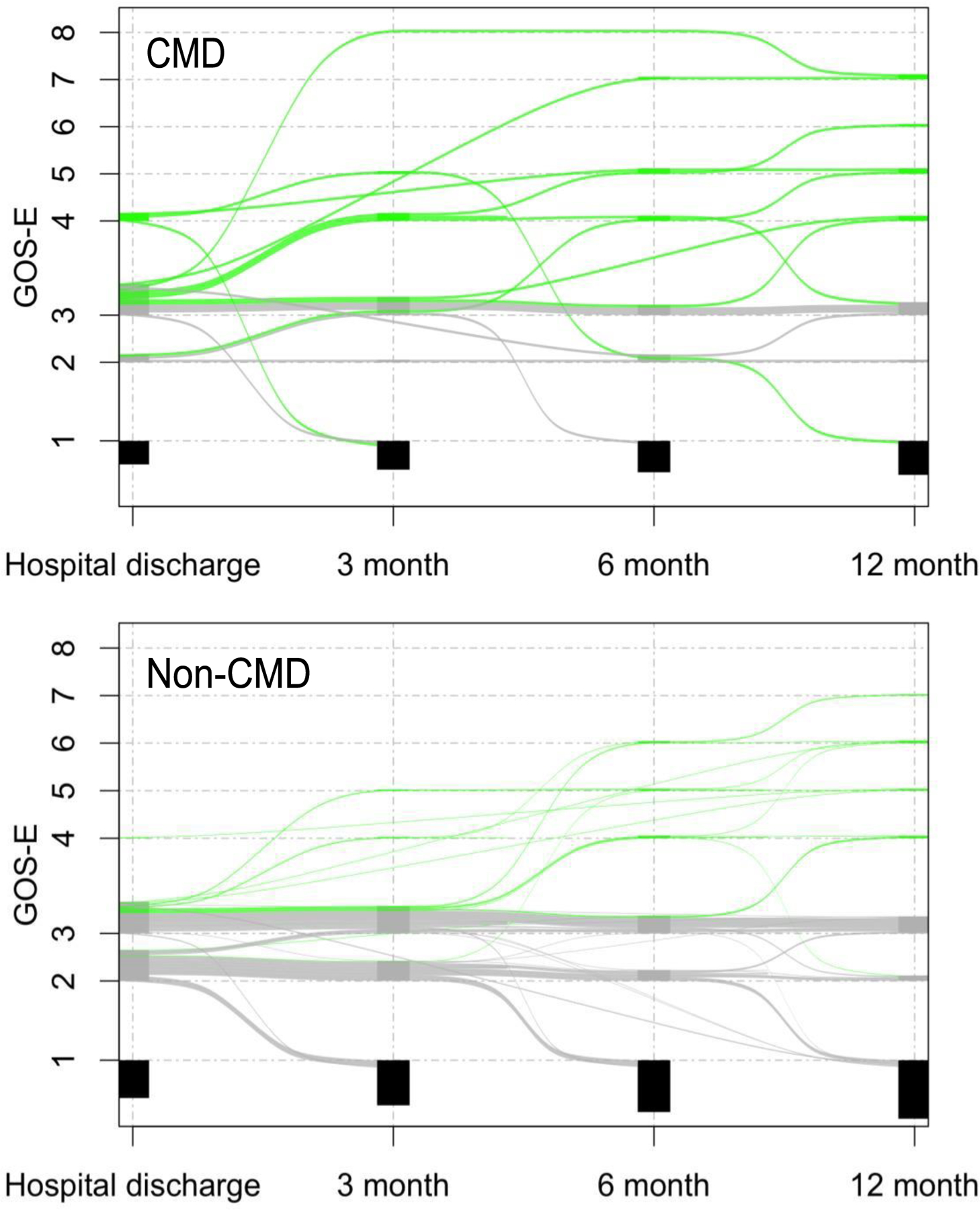
Methods: In this observational cohort study, we prospectively studied two independent cohorts of clinically unresponsive patients (aged ≥18 years) with acute brain injury. Machine learning was applied to EEG recordings to diagnose cognitive-motor dissociation by detecting brain activation in response to verbal commands. Survival statistics and shift analyses were applied to the data to identify an association between cognitive-motor dissociation and time to and magnitude of recovery. The prediction accuracy of the model that was built using the derivation cohort was assessed using the validation cohort. Functional outcomes of all patients were assessed with the Glasgow Outcome Scale-Extended (GOS-E) at hospital discharge and at 3, 6, and 12 months after injury. Patients who underwent withdrawal of life-sustaining therapies were censored, and death was treated as a competing risk.
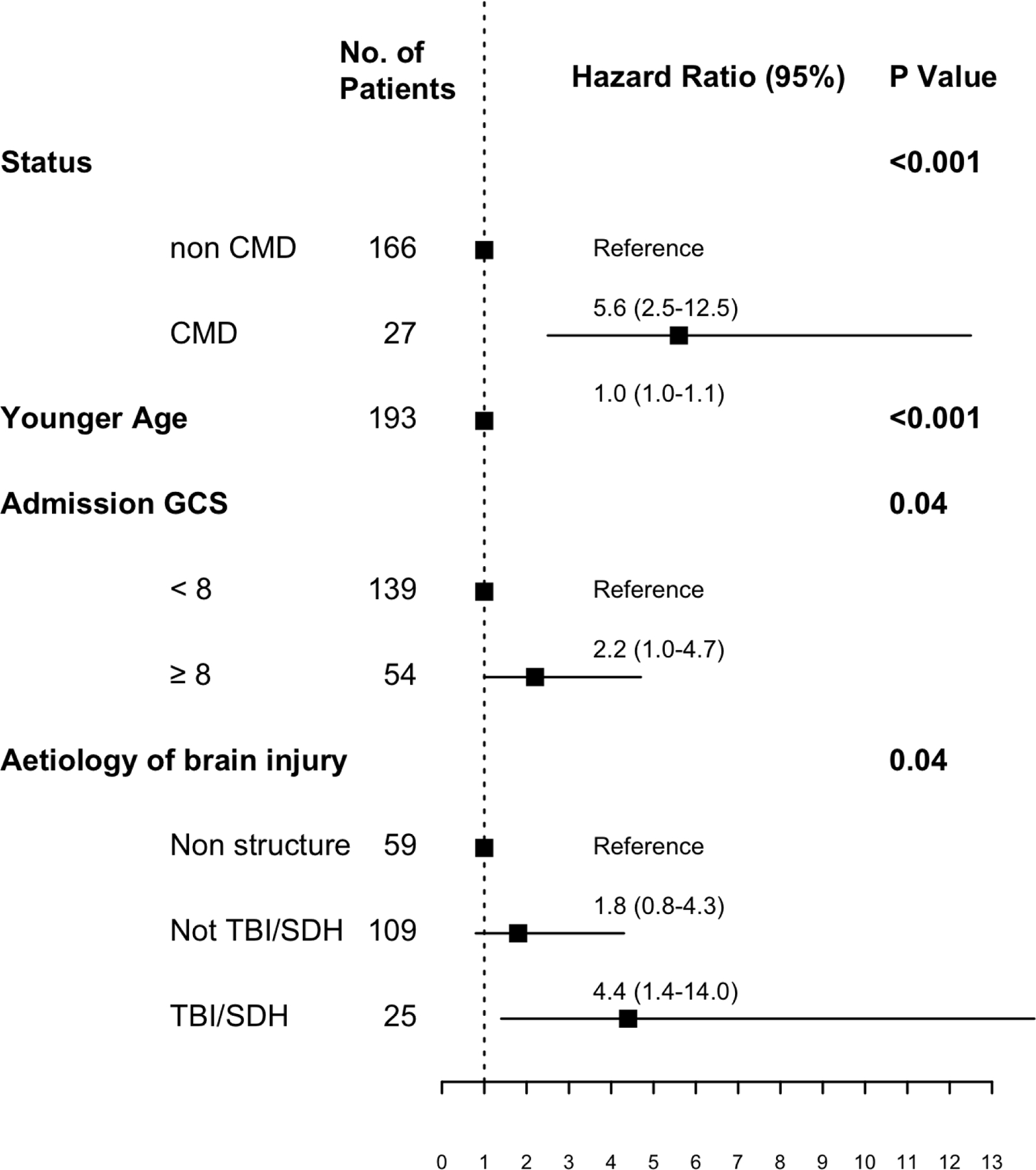
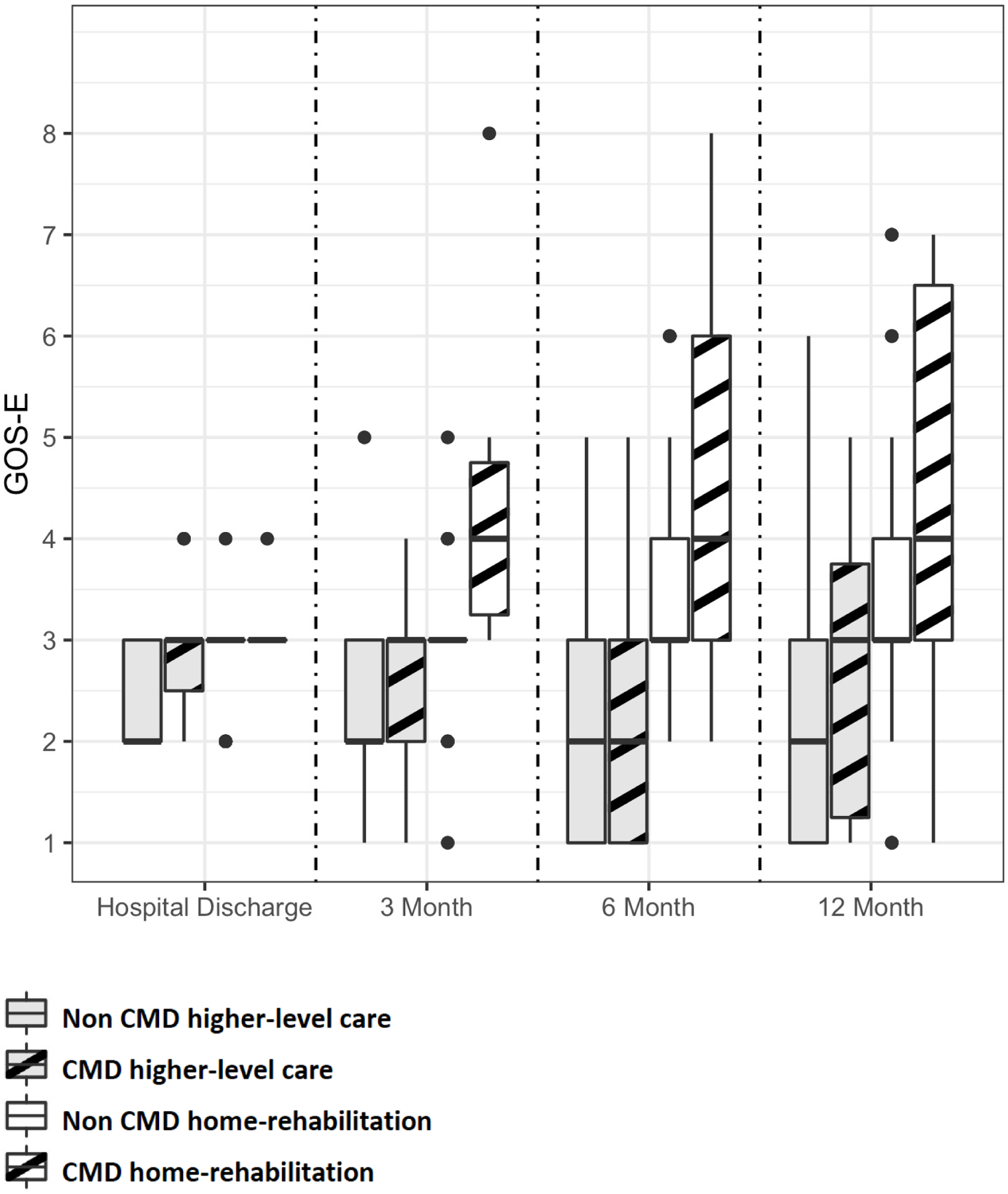
Findings: Between July 1, 2014, and Sept 30, 2021, we screened 598 patients with acute brain injury and included 193 (32%) patients, of whom 100 were in the derivation cohort and 93 were in the validation cohort. At 12 months, 28 (15%) of 193 unresponsive patients had a GOS-E score of 4 or above. Cognitive-motor dissociation was seen in 27 (14%) patients and was an independent predictor of shorter time to good recovery (hazard ratio 5·6 [95% CI 2·5-12·5]), as was underlying traumatic brain injury or subdural haematoma (4·4 [1·4-14·0]), a Glasgow Coma Scale score on admission of greater than or equal to 8 (2·2 [1·0-4·7]), and younger age (1·0 [1·0-1·1]). Among patients discharged home or to a rehabilitation setting, those diagnosed with cognitive-motor dissociation consistently had higher scores on GOS-E indicating better functional recovery compared with those without cognitive-motor dissociation, which was seen as early as 3 months after the injury (odds ratio 4·5 [95% CI 2·0-33·6]).
Interpretation: Recovery trajectories of clinically unresponsive patients diagnosed with cognitive-motor dissociation early after brain injury are distinctly different from those without cognitive-motor dissociation. A diagnosis of cognitive-motor dissociation could inform the counselling of families of clinically unresponsive patients, and it could help clinicians to identify patients who will benefit from rehabilitation.
Funding: US National Institutes of Health.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests DR is supported by grant funding from the US National Institutes of Health (NIH; HL151901). SA is supported by grant funding from the NIH (HL153311). SP is supported by grant funding from the NIH (NS113055). JC is a minority shareholder at iCE Neurosystems and is supported by grant funding from the NIH (NS106014, NS112760), and the McDonnell Foundation. All other authors declare no competing interests.
Figures

Comment in
-
Improving prognostication after severe brain injury.Lancet Neurol. 2022 Aug;21(8):673-674. doi: 10.1016/S1474-4422(22)00262-9. Lancet Neurol. 2022. PMID: 35841896 No abstract available.
References
-
- Jourdan C, Bayen E, Bosserelle V, et al. Referral to rehabilitation after severe traumatic brain injury: Results from the PariS-TBI study. Neurorehabil Neural Repair 2013;27(1):35–44. - PubMed
-
- Katz DI, Polyak M, Coughlan D, Nichols M, Roche A. Natural history of recovery from brain injury after prolonged disorders of consciousness: outcome of patients admitted to inpatient rehabilitation with 1–4 year follow-up. Prog Brain Res 2009;177:73–88. - PubMed
-
- Estraneo A, Moretta P, Loreto V, Lanzillo B, Santoro L, Trojano L. Late recovery after traumatic, anoxic, or hemorrhagic long-lasting vegetative state. Neurology 2010;75(3):239–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
