

A retrospective descriptive analysis of non-physician-performed prehospital endotracheal intubation practices and performance in South Africa
- PMID: 35842578
- PMCID: PMC9287876
- DOI: 10.1186/s12873-022-00688-4
A retrospective descriptive analysis of non-physician-performed prehospital endotracheal intubation practices and performance in South Africa
Abstract
Introduction: Prehospital advanced airway management, including endotracheal intubation (ETI), is one of the most commonly performed advanced life support skills. In South Africa, prehospital ETI is performed by non-physician prehospital providers. This practice has recently come under scrutiny due to lower first pass (FPS) and overall success rates, a high incidence of adverse events (AEs), and limited evidence regarding the impact of ETI on mortality. The aim of this study was to describe non-physician ETI in a South African national sample in terms of patient demographics, indications for intubation, means of intubation and success rates. A secondary aim was to determine what factors were predictive of first pass success.
Methods: This study was a retrospective chart review of prehospital ETIs performed by non-physician prehospital providers, between 01 January 2017 and 31 December 2017. Two national private Emergency Medical Services (EMS) and one provincial public EMS were sampled. Data were analysed descriptively and summarised. Logistic regression was performed to evaluate factors that affect the likelihood of FPS.
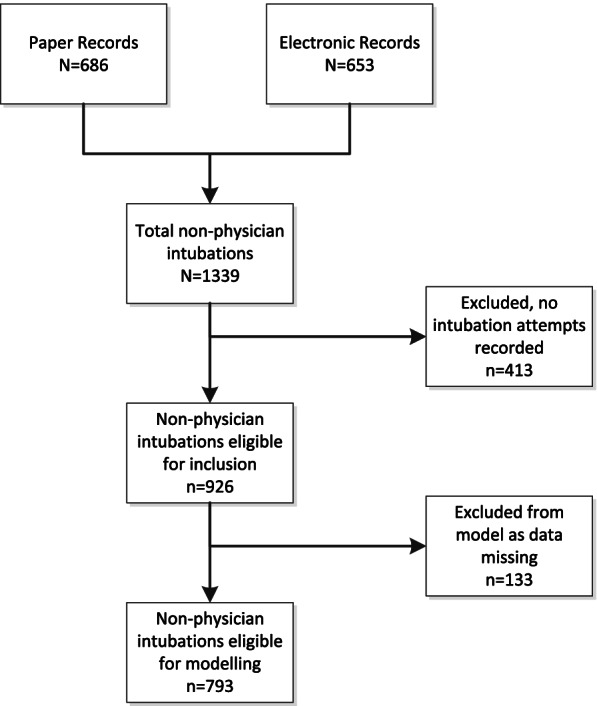
Results: A total of 926 cases were included. The majority of cases were adults (n = 781, 84.3%) and male (n = 553, 57.6%). The most common pathologies requiring emergency treatment were head injury, including traumatic brain injury (n = 328, 35.4%), followed by cardiac arrest (n = 204, 22.0%). The mean time on scene was 46 minutes (SD = 28.3). The most cited indication for intubation was decreased level of consciousness (n = 515, 55.6%), followed by cardiac arrest (n = 242, 26.9%) and ineffective ventilation (n = 96, 10.4%). Rapid sequence intubation (RSI, n = 344, 37.2%) was the most common approach. The FPS rate was 75.3%, with an overall success rate of 95.7%. Intubation failed in 33 (3.6%) patients. The need for ventilation was inversely associated with FPS (OR = 0.42, 95% CI: 0.20-0.88, p = 0.02); while deep sedation (OR = 0.56, 95% CI: 0.36-0.88, p = 0.13) and no drugs (OR = 0.47, 95% CI: 0.25-0.90, p = 0.02) compared to RSI was less likely to result in FPS. Increased scene time (OR = 0.99, 95% CI: 0.985-0.997, p < 0.01) was inversely associated FPS.
Conclusion: This is one of the first and largest studies evaluating prehospital ETI in Africa. In this sample of ground-based EMS non-physician ETI, we found success rates similar to those reported in the literature. More research is needed to determine AE rates and the impact of ETI on patient outcome. There is an urgent need to standardise prehospital ETI reporting in South Africa to facilitate future research.
Keywords: Airway management; Endotracheal intubation; Prehospital emergency care; South Africa.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
