

Exploring immunotherapy in colorectal cancer
- PMID: 35842707
- PMCID: PMC9288068
- DOI: 10.1186/s13045-022-01294-4
Exploring immunotherapy in colorectal cancer
Abstract
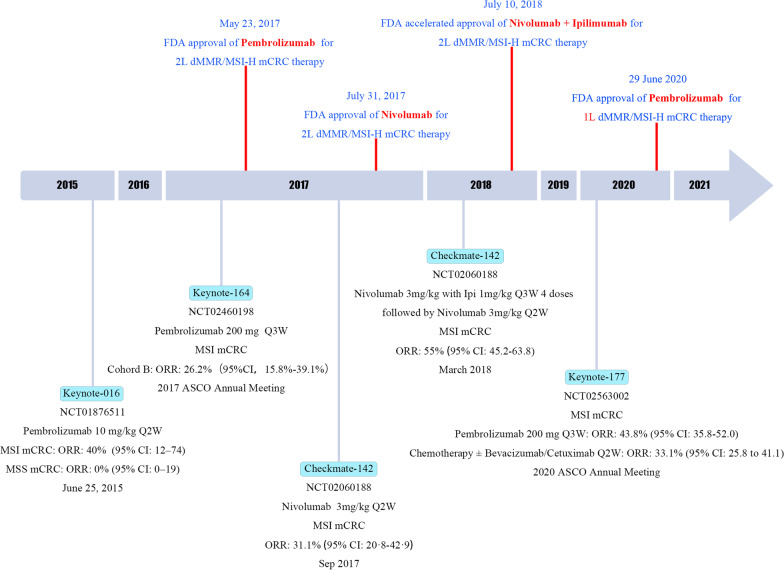
Chemotherapy combined with or without targeted therapy is the fundamental treatment for metastatic colorectal cancer (mCRC). Due to the adverse effects of chemotherapeutic drugs and the biological characteristics of the tumor cells, it is difficult to make breakthroughs in traditional strategies. The immune checkpoint blockades (ICB) therapy has made significant progress in the treatment of advanced malignant tumors, and patients who benefit from this therapy may obtain a long-lasting response. Unfortunately, immunotherapy is only effective in a limited number of patients with microsatellite instability-high (MSI-H), and segment initial responders can subsequently develop acquired resistance. From September 4, 2014, the first anti-PD-1/PD-L1 drug Pembrolizumab was approved by the FDA for the second-line treatment of advanced malignant melanoma. Subsequently, it was approved for mCRC second-line treatment in 2017. Immunotherapy has rapidly developed in the past 7 years. The in-depth research of the ICB treatment indicated that the mechanism of colorectal cancer immune-resistance has become gradually clear, and new predictive biomarkers are constantly emerging. Clinical trials examining the effect of immune checkpoints are actively carried out, in order to produce long-lasting effects for mCRC patients. This review summarizes the treatment strategies for mCRC patients, discusses the mechanism and application of ICB in mCRC treatment, outlines the potential markers of the ICB efficacy, lists the key results of the clinical trials, and collects the recent basic research results, in order to provide a theoretical basis and practical direction for immunotherapy strategies.
Keywords: Biomarkers; Immune checkpoint blockade; Immune desert; Immunotherapy; Metastatic colorectal cancer; Microsatellite instability; Precision medicine.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- The National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology, Rectal Cancer. Version 3.2021, <https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf> (2021). - PubMed
-
- The National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology, Colon Cancer. Version 2.2021, <https://www.nccn.org/professionals/physician_gls/pdf/colon.pdfc> ( 2021).
-
- ESMO consensus guidelines for the management of patients with metastatic colorectal cancer, <https://www.annalsofoncology.org/article/S0923-7534(19)34754-4/pdf> (2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
