

COVID-19: gastrointestinal and hepatobiliary manifestations
- PMID: 35843340
- PMCID: PMC9288242
- DOI: 10.1016/j.humpath.2022.07.006
COVID-19: gastrointestinal and hepatobiliary manifestations
Abstract
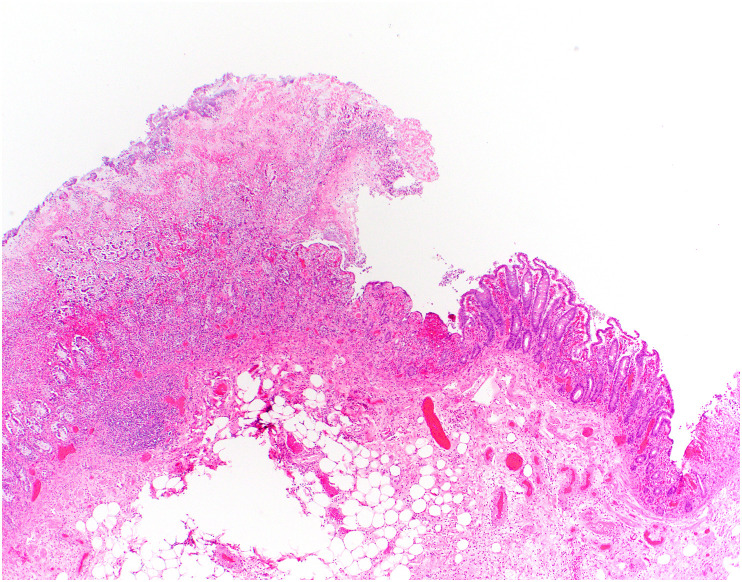
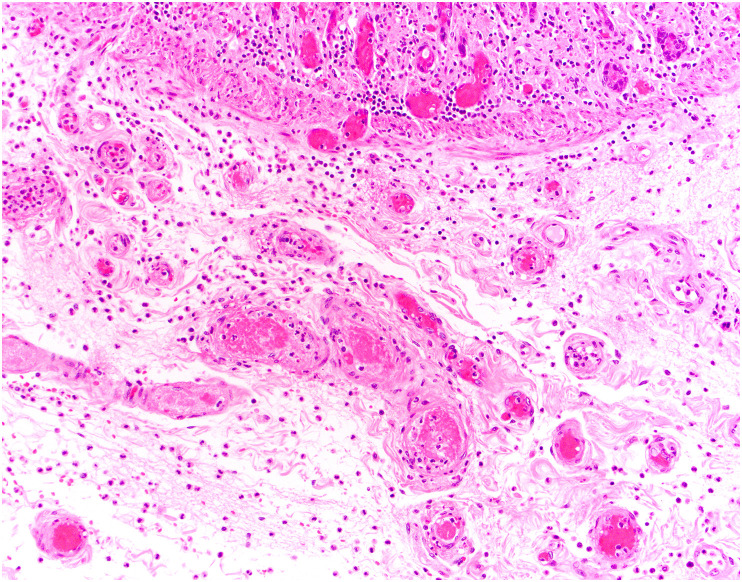
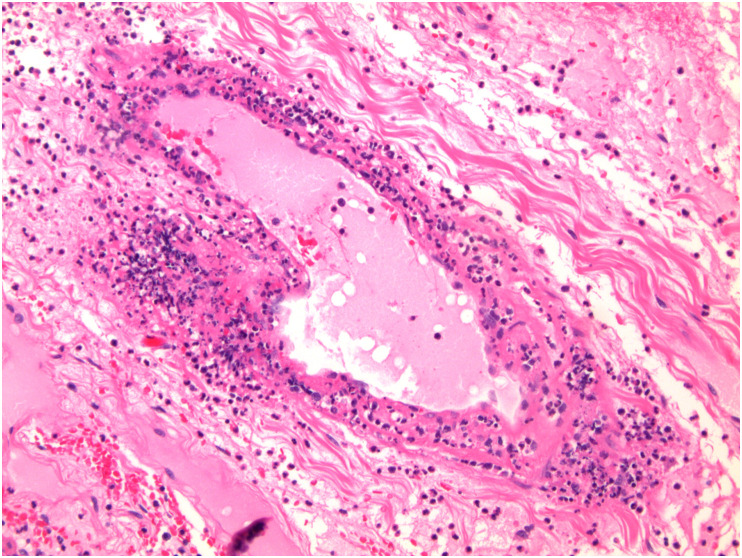
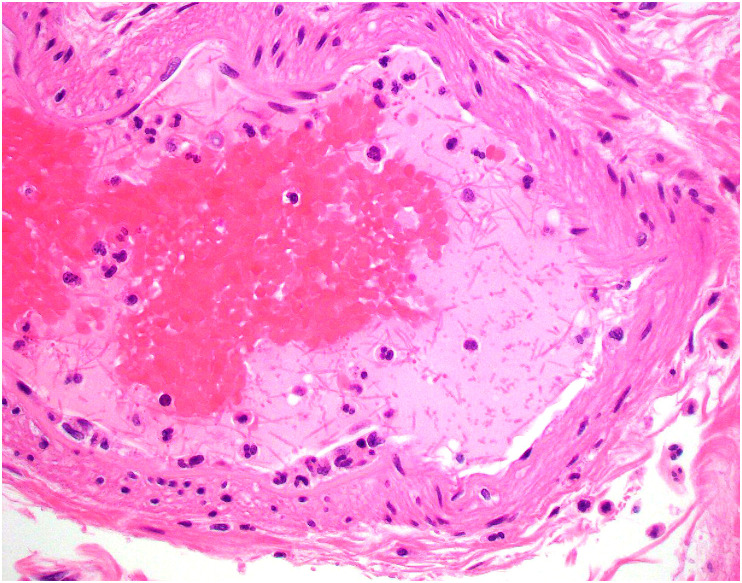
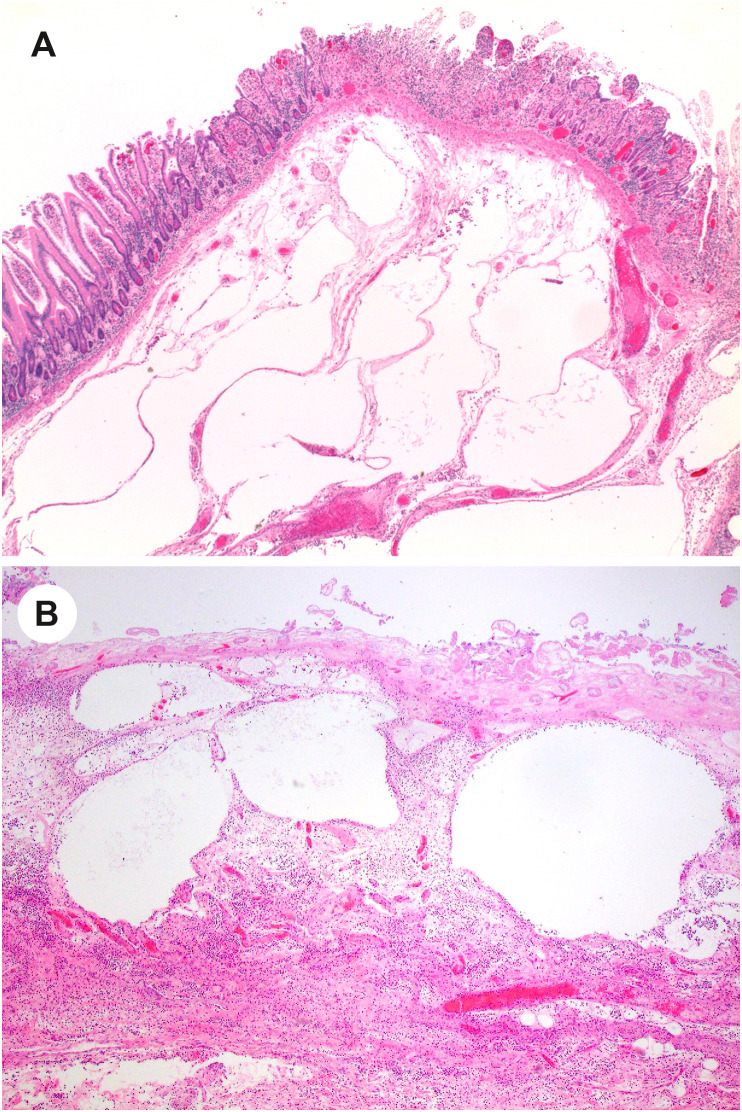
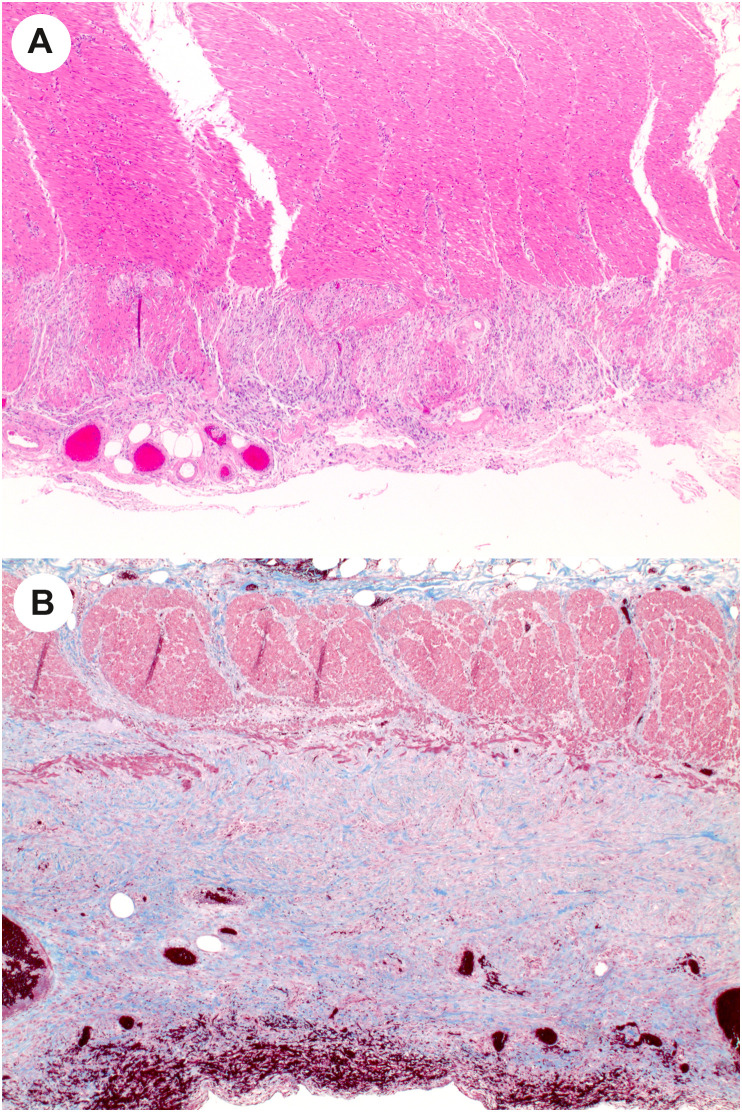
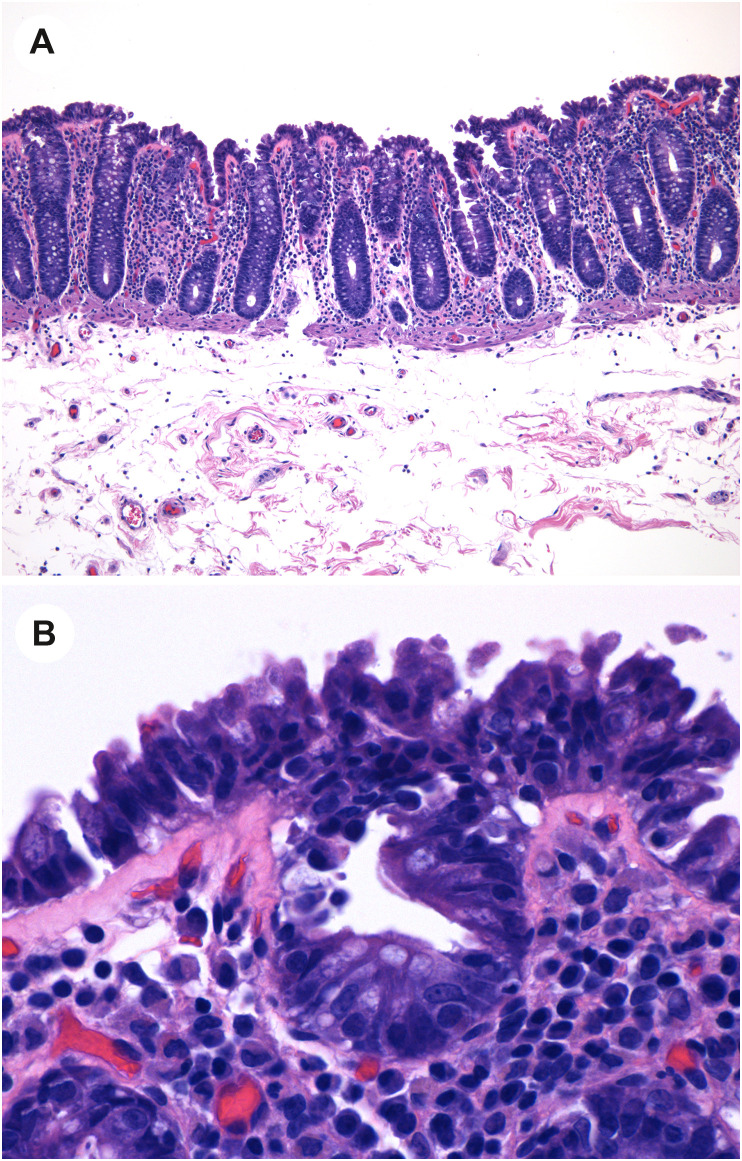
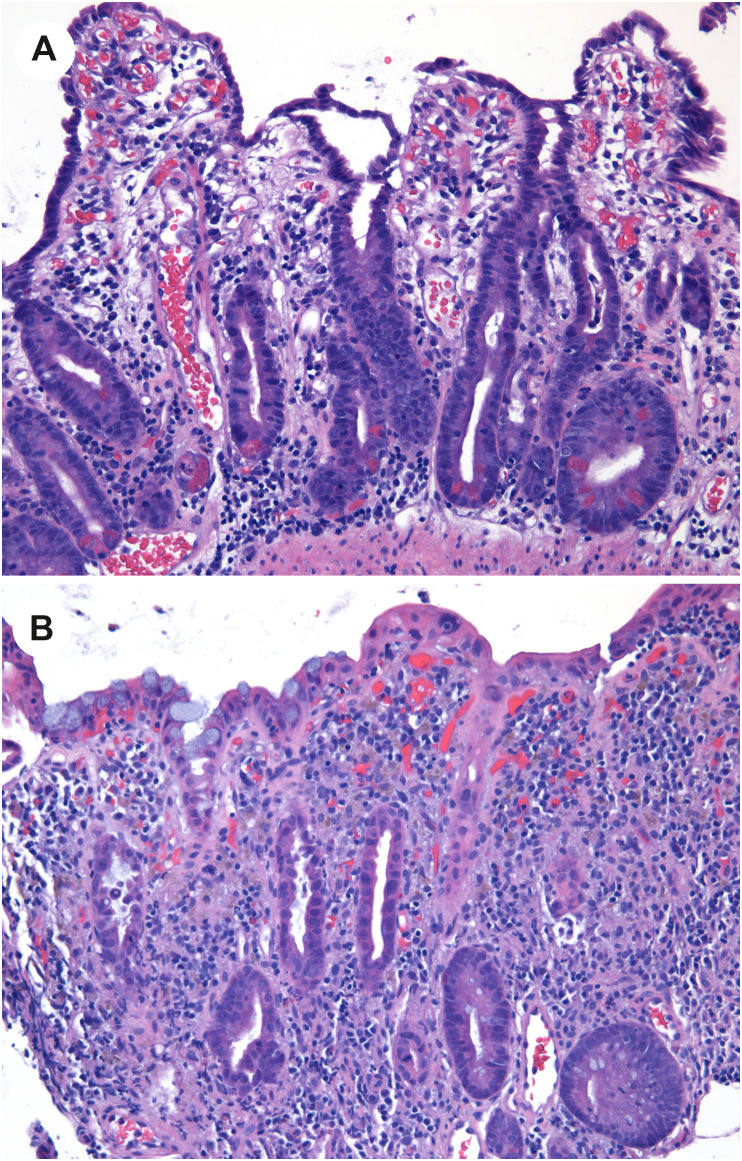
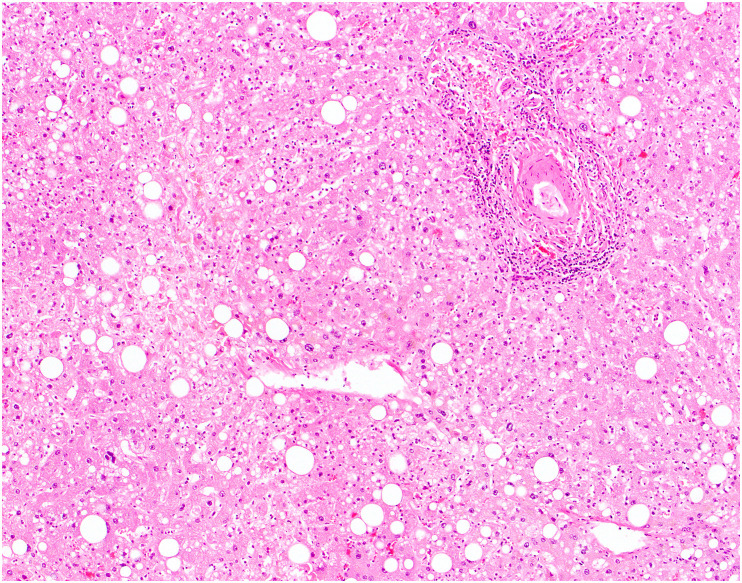
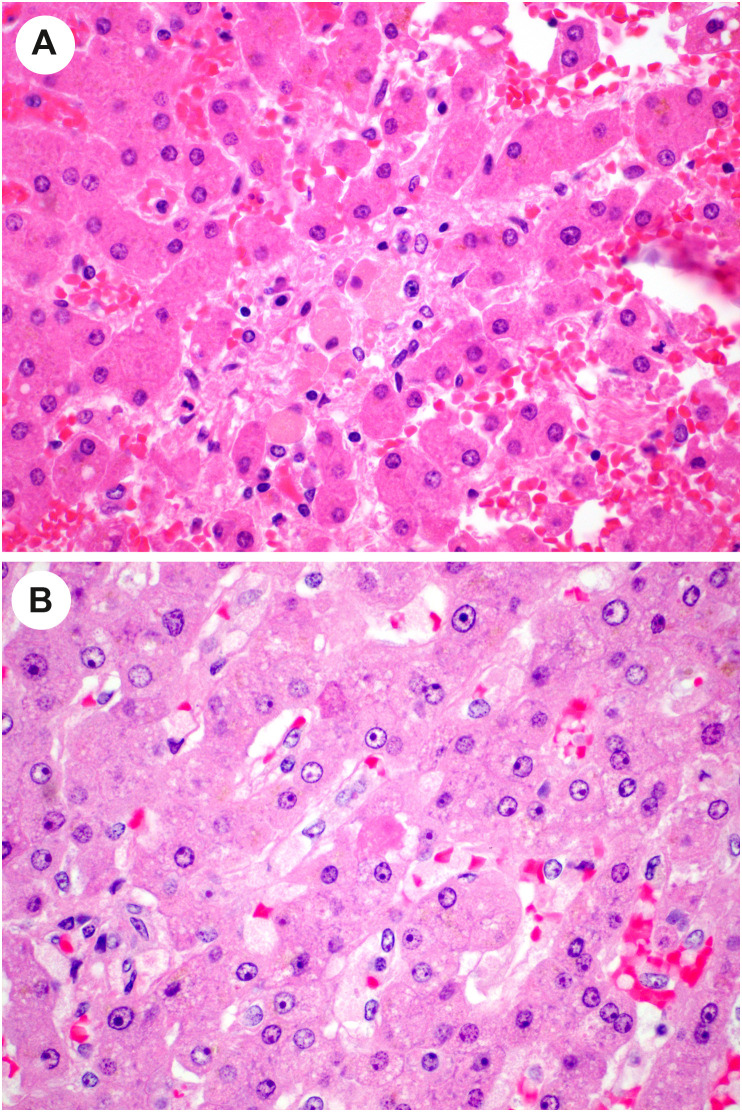
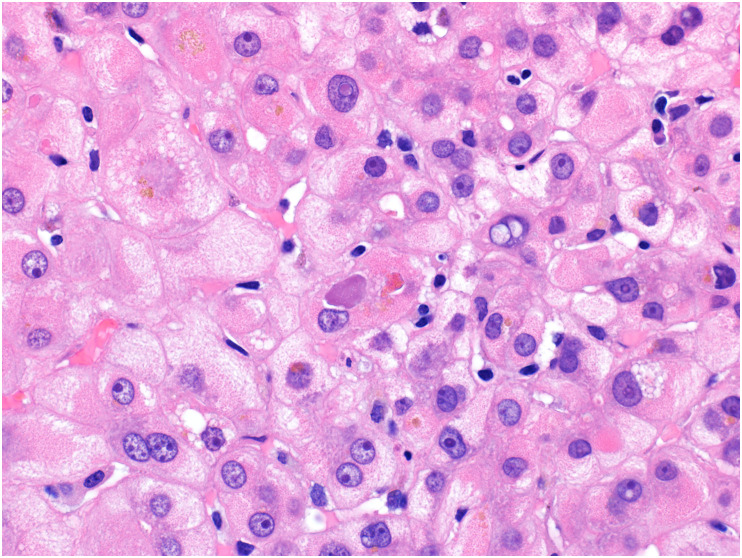
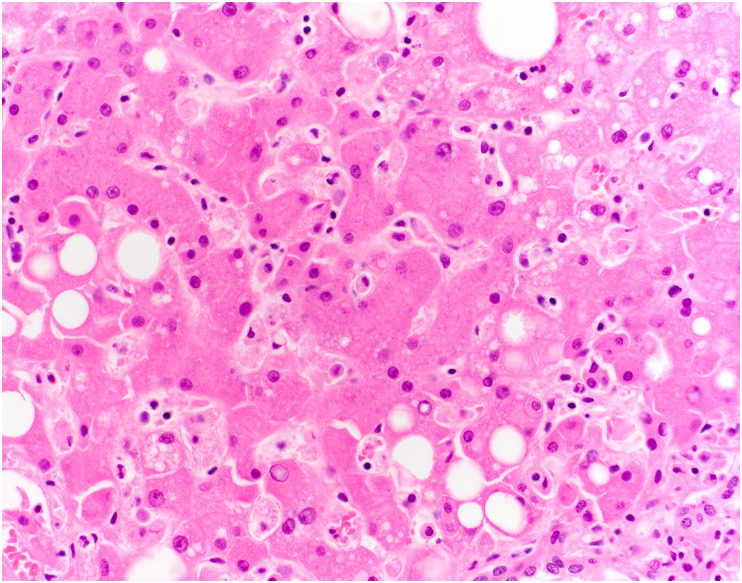
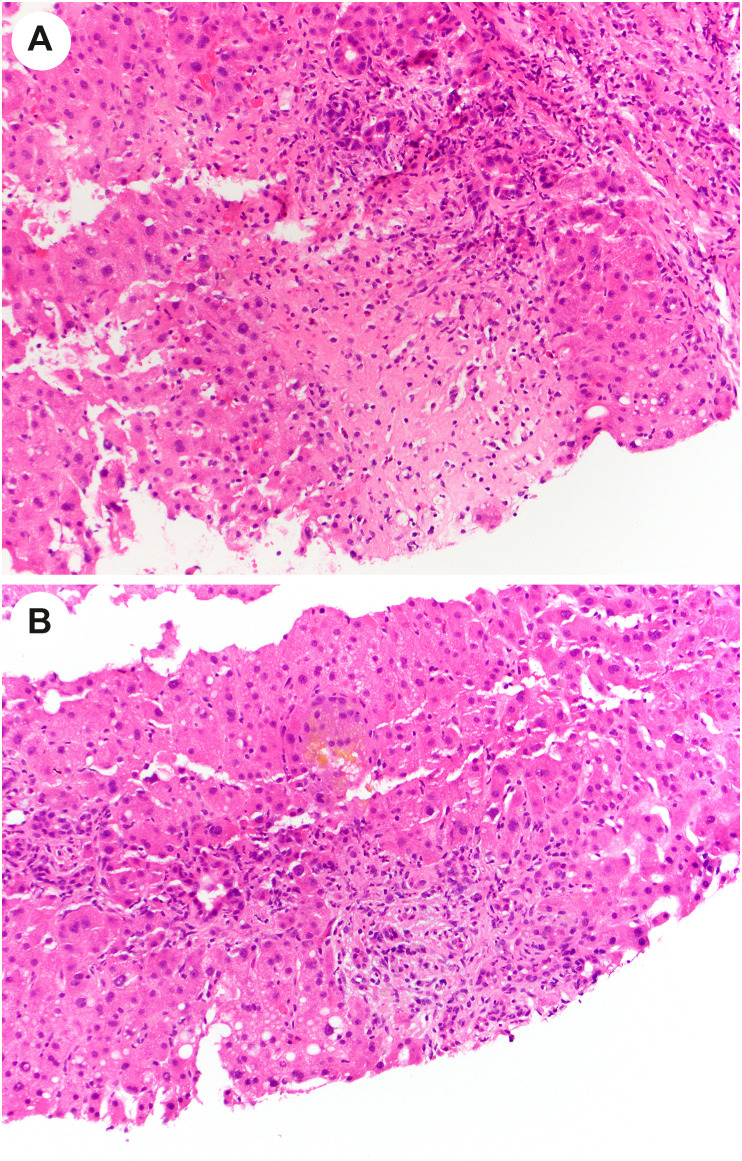
SARS-CoV-2 is the viral agent of COVID-19, a pandemic that surfaced in 2019. Although predominantly a respiratory ailment, patients with COVID-19 can have gastrointestinal (GI) and hepatobiliary manifestations. These manifestations are often mild and transient, but they can be severe and consequential. In the GI tract, ischemic enterocolitis is the most common and significant consequence of COVID-19. In the liver, the reported pathologic findings may often be related to consequences of severe systemic viral infection, but reports of hepatitis presumed to be due to SARS-CoV-2 suggest that direct viral infection of the liver may be a rare complication of COVID-19. In both the GI tract and liver, lingering symptoms of GI or hepatic injury after resolution of pulmonary infection may be part of the evolving spectrum of long COVID.
Keywords: COVID-19; Colon; Gastrointestinal; Liver; Pathology.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
