Association of transport time interval with neurologic outcome in out-of-hospital cardiac arrest patients without return of spontaneous circulation on scene and the interaction effect according to prehospital airway management
- PMID: 35843609
- PMCID: PMC9288882
- DOI: 10.15441/ceem.21.074
Association of transport time interval with neurologic outcome in out-of-hospital cardiac arrest patients without return of spontaneous circulation on scene and the interaction effect according to prehospital airway management
Abstract
Objective: This study analyzed the association of transport time interval (TTI) with survival rate and neurologic outcome in out-of-hospital cardiac arrest (OHCA) patients without return of spontaneous circulation (ROSC) and the interaction effect of TTI according to prehospital airway management.
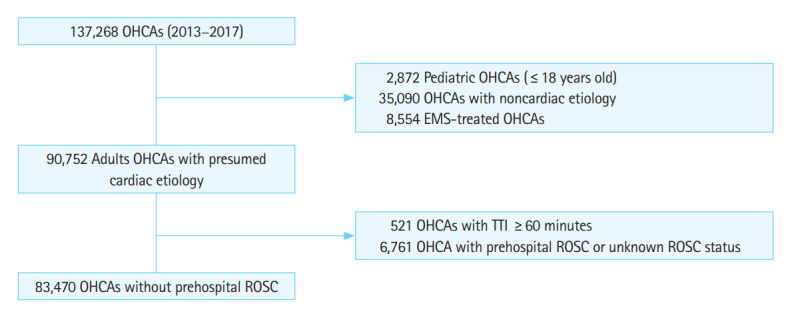
Methods: A retrospective observational study based on the nationwide OHCA database from January 2013 to December 2017 was designed. Emergency medical service (EMS)-treated OHCA patients aged ≥18 years were included. TTI was categorized into four groups of quartiles (≤4, 5-7, 8-11, ≥12 minutes). The primary outcome was favorable neurologic outcome at discharge. The secondary outcome was survival to discharge from the hospital. Multivariable logistic regression was used to analyze outcomes according to TTI. A different effect of TTI according to the administration of prehospital EMS advanced airway was evaluated.
Results: In total, 83,470 patients were analyzed. Good neurologic recovery decreased as TTI increased (1.0% for TTI ≤4 minutes, 0.9% for TTI 5-7 minutes, 0.6% for TTI 8-11 minutes, and 0.5% for TTI ≥12 minutes; P for trend <0.05). The adjusted odds ratio of prolonged TTI (≥12 minutes) was 0.73 (95% confidence interval, 0.57-0.93; P<0.01) for good neurologic recovery. However, the negative effect of prolonged TTI on neurological outcome was insignificant when advanced airway or entotracheal intubation were performed by EMS providers (adjusted odds ratio, 1.17; 95% confidence interval, 0.42-3.29; P=0.76).
Conclusion: EMS TTI was negatively associated with the neurologic outcome of OHCA without ROSC on scene. When advanced airway was performed on scene, TTI was insignificantly associated with the outcome.
Keywords: Emergency medical services; Heart arrest; Intubation.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
The Effect of Transport Time Interval on Neurological Recovery after Out-of-Hospital Cardiac Arrest in Patients without a Prehospital Return of Spontaneous Circulation.J Korean Med Sci. 2019 Feb 28;34(9):e73. doi: 10.3346/jkms.2019.34.e73. eCollection 2019 Mar 11. J Korean Med Sci. 2019. PMID: 30863269 Free PMC article.
-
Association of prehospital airway management technique with survival outcomes of out-of-hospital cardiac arrest patients.PLoS One. 2022 Jun 6;17(6):e0269599. doi: 10.1371/journal.pone.0269599. eCollection 2022. PLoS One. 2022. PMID: 35666760 Free PMC article.
-
Association between the number of prehospital defibrillation attempts and neurologic outcomes in out-of-hospital cardiac arrest patients without on-scene return of spontaneous circulation.Clin Exp Emerg Med. 2021 Mar;8(1):21-29. doi: 10.15441/ceem.20.069. Epub 2021 Mar 31. Clin Exp Emerg Med. 2021. PMID: 33845519 Free PMC article.
-
Location of arrest and effect of prehospital advanced airway management after emergency medical service-witnessed out-of-hospital cardiac arrest: nationwide observational study.Emerg Med J. 2019 Sep;36(9):541-547. doi: 10.1136/emermed-2018-207871. Epub 2019 Jul 20. Emerg Med J. 2019. PMID: 31326952
-
Endotracheal intubation versus supraglottic airway placement in out-of-hospital cardiac arrest: A meta-analysis.Resuscitation. 2015 Aug;93:20-6. doi: 10.1016/j.resuscitation.2015.05.007. Epub 2015 May 23. Resuscitation. 2015. PMID: 26006743 Review.
Cited by
-
Advanced age and neurological recovery in elderly patients with out-of-hospital cardiac arrest treated with targeted temperature management: a nationwide population‑based registry study 2016-2020.Intern Emerg Med. 2025 Jan;20(1):281-289. doi: 10.1007/s11739-024-03662-z. Epub 2024 Jun 7. Intern Emerg Med. 2025. PMID: 38847959
-
Current trends in emergency airway management: a clinical review.Clin Exp Emerg Med. 2024 Sep;11(3):243-258. doi: 10.15441/ceem.23.173. Epub 2024 Mar 15. Clin Exp Emerg Med. 2024. PMID: 38485262 Free PMC article.
-
Machine learning pre-hospital real-time cardiac arrest outcome prediction (PReCAP) using time-adaptive cohort model based on the Pan-Asian Resuscitation Outcome Study.Sci Rep. 2023 Nov 21;13(1):20344. doi: 10.1038/s41598-023-45767-z. Sci Rep. 2023. PMID: 37990066 Free PMC article.
-
Out-of-hospital cardiac arrest outcomes' determinants: an Italian retrospective cohort study based on Lombardia CARe.Intern Emerg Med. 2024 Oct;19(7):2035-2045. doi: 10.1007/s11739-024-03573-z. Epub 2024 Mar 28. Intern Emerg Med. 2024. PMID: 38548967 Free PMC article.
-
Validation of the Termination of Resuscitation Rules in Detroit.Cureus. 2025 Feb 28;17(2):e79846. doi: 10.7759/cureus.79846. eCollection 2025 Feb. Cureus. 2025. PMID: 40161053 Free PMC article.
References
-
- Ong ME, Shin SD, De Souza NN, et al. Outcomes for out-of-hospital cardiac arrests across 7 countries in Asia: the Pan Asian Resuscitation Outcomes Study (PAROS) Resuscitation. 2015;96:100–8. - PubMed
-
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81:1479–87. - PubMed
-
- Neumar RW, Shuster M, Callaway CW, et al. Part 1: executive summary. 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S315–67. - PubMed
-
- Kajino K, Iwami T, Daya M, et al. Impact of transport to critical care medical centers on outcomes after out-of-hospital cardiac arrest. Resuscitation. 2010;81:549–54. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources