Time on shift in the emergency department and decision to prescribe opioids to patients without chronic opioid use
- PMID: 35843610
- PMCID: PMC9288880
- DOI: 10.15441/ceem.22.212
Time on shift in the emergency department and decision to prescribe opioids to patients without chronic opioid use
Abstract
Objective: To study the effect of time on shift on the opioid prescribing practices of emergency physicians among patients without chronic opioid use.
Methods: We analyzed pain-related visits for five painful conditions from 2010 to 2017 at a single academic hospital in Boston. Visits were categorized according to national guidelines as conditions for which opioids are "sometimes indicated" (fracture and renal colic) or "usually not indicated" (headache, low back pain, and fibromyalgia). Using conditional logistic regression with fixed effects for clinicians, we estimated the probability of opioid prescribing for pain-related visits as a function of shift hour at discharge, time of day, and patient-level confounders (age, sex, and pain score).
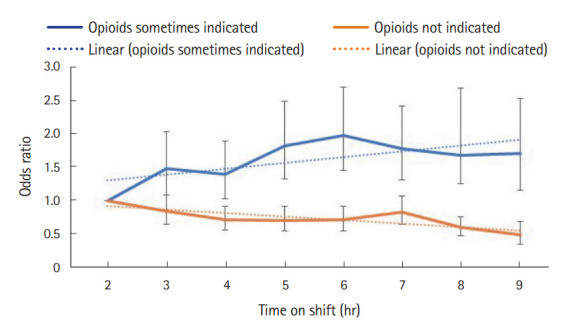
Results: Among 16,115 visits for which opioids were sometimes indicated, opioid prescribing increased over the course of a shift (28% in the first hour compared with 40% in the last hour; adjusted odds ratio, 1.06; 95% confidence interval, 1.02-1.10; adjusted P-trend <0.01). However, among visits for which opioids are usually not indicated, relative to the first hour, opioid prescriptions progressively fell (40% in the first hour compared with 23% in the last hour; adjusted odds ratio, 0.93; 95% confidence interval, 0.91-0.96; adjusted P-trend <0.01).
Conclusion: As shift hour progressed, emergency physicians became more likely to prescribe opioids for conditions that are sometimes indicated, and less likely to prescribe opioids for nonindicated conditions. Our study suggests that clinical decision making in the emergency department can be substantially influenced by external factors such as clinician shift hour.
Keywords: Decision making; Operations research; Opioid analgesics.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Beaudoin FL, Straube S, Lopez J, Mello MJ, Baird J. Prescription opioid misuse among ED patients discharged with opioids. Am J Emerg Med. 2014;32:580–5. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials