

Postmenopausal hyperandrogenism due to an ovarian sex cord-stromal tumour causing elevated dehydroepiandrosterone sulphate: a case report
- PMID: 35843927
- PMCID: PMC9288717
- DOI: 10.1186/s12905-022-01879-8
Postmenopausal hyperandrogenism due to an ovarian sex cord-stromal tumour causing elevated dehydroepiandrosterone sulphate: a case report
Abstract
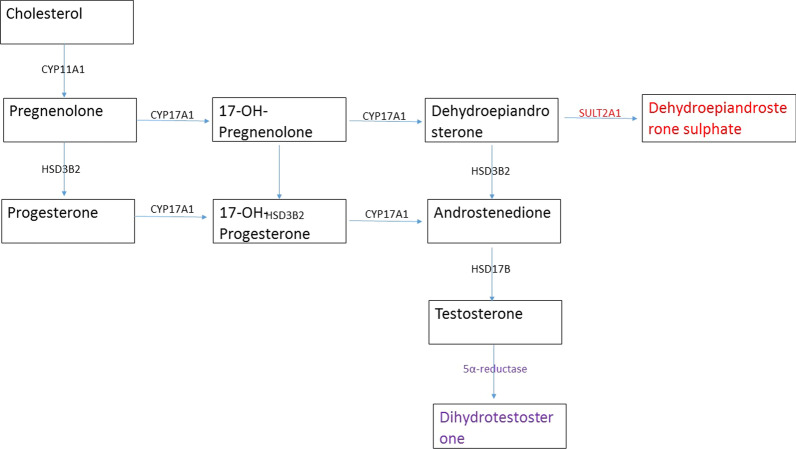
Background: The source of excess androgen can be obscure in postmenopausal women with new-onset hyperandrogenism. If serum dehydroepiandrosterone sulphate (DHEAS) is raised, it is presumed to be of adrenal origin because DHEAS is exclusively produced from adrenal cortical cells. This reports an elderly female presenting with new-onset hyperandrogenism due to an ovarian sex cord-stromal tumour, associated with increased serum DHEAS levels.
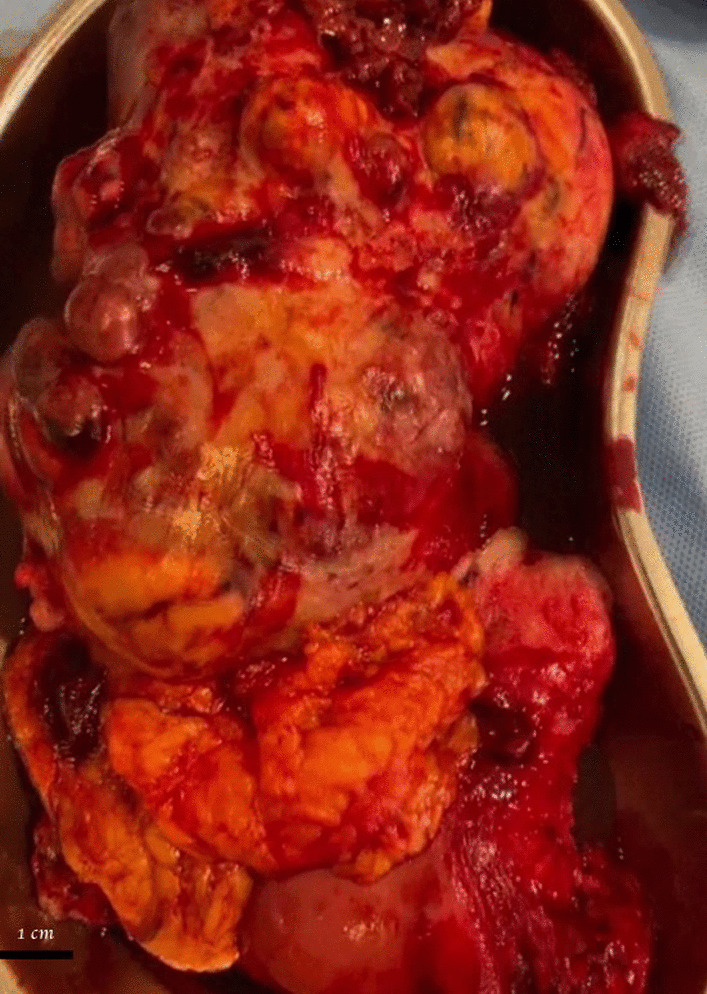
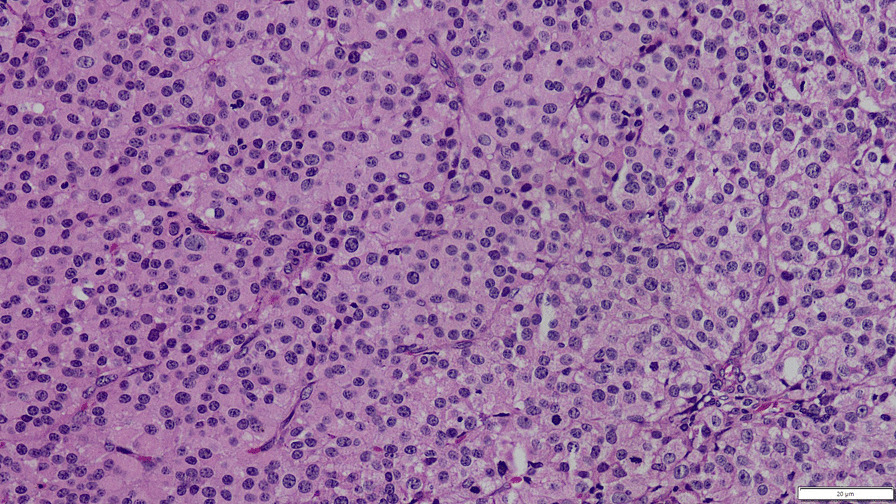
Case description: A 76-year-old female with long-standing diabetes and hypertension presented with hirsutism and male type alopecia for six months. She had menopause at 55 years of age. There was a pelvic mass on examination. Total testosterone was 6.106 ng/ml (0.124-0.357) and DHEAS was > 1000 µg/dL (35-430). Contrast-enhanced computed tomography of the abdomen and pelvis showed a heterogeneously enhancing complex mass measuring 11 × 8 cm in the left adnexal region. Adrenal glands were normal. She underwent total abdominal hysterectomy, bilateral salphingo-oophorectomy, and omentectomy. Both testosterone and DHEAS normalised following surgery. Histology revealed a sex cord-stromal tumour, likely a steroid cell tumour with malignant potential. Fluorodeoxyglucose-Positron emission tomography did not show any additional lesions.
Conclusions: Due to the lack of sulfotransferase in ovarian tissue, markedly elevated DHEAS originating from an ovarian neoplasm is unusual. This phenomenon has not been described except in a patient with a steroid cell tumour causing Cushing syndrome and hyperandrogenism. The mechanism of this rare occurrence remains elusive. Knowledge of this unusual presentation would enable the clinicians to be cautious in localising the androgen source in women with hyperandrogenism.
Keywords: DHEAS; Dehydroepiandrosterone sulphate; Hyperandrogenism; Ovary; Sex cord-stromal tumour.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Morgan LS. Hormonally active gynecologic tumors. In: Seminars in surgical oncology. Wiley Online Library; 1990. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
