

Rituximab Therapy for Mucous Membrane Pemphigoid: A Retrospective Monocentric Study With Long-Term Follow-Up in 109 Patients
- PMID: 35844526
- PMCID: PMC9281543
- DOI: 10.3389/fimmu.2022.915205
Rituximab Therapy for Mucous Membrane Pemphigoid: A Retrospective Monocentric Study With Long-Term Follow-Up in 109 Patients
Abstract
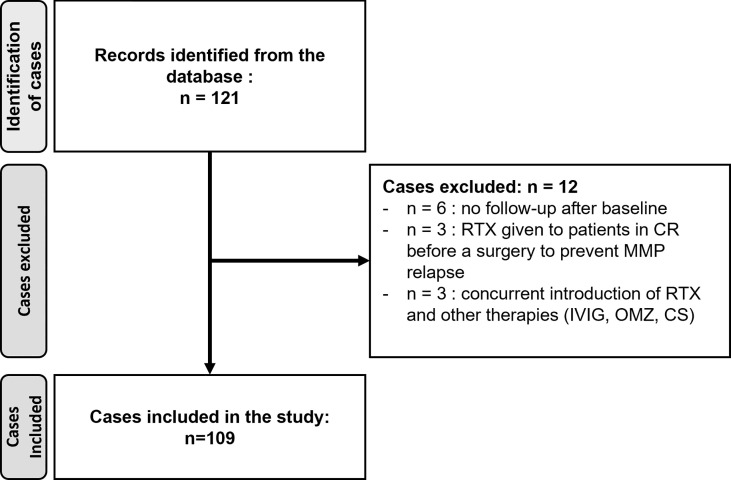
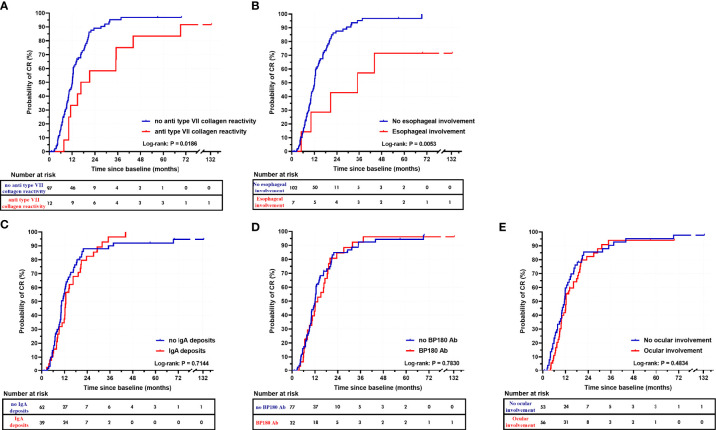
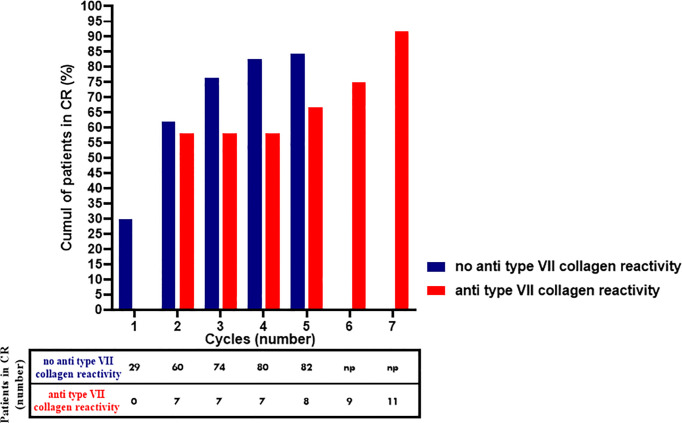
Mucous membrane pemphigoid (MMP) is a heterogeneous group of rare, chronic, subepithelial autoimmune blistering diseases (AIBDs) with predominant involvement of mucous membranes that can be sight-threatening and life-threatening. Rituximab (RTX) has demonstrated its efficacy in severe MMP refractory to conventional immunosuppressants in small series that differed in RTX scheme, concomitant therapies, and outcome definitions. In a meta-analysis involving 112 patients with MMP treated with RTX, complete remission (CR) was reported in 70.5% of cases. Herein, we report the largest retrospective monocentric study on RTX efficacy in a series of 109 severe and/or refractory patients with MMP treated with RTX with a median follow-up period of 51.4 months. RTX was administered in association with immunomodulatory drugs (dapsone, salazopyrine) without any other systemic immunosuppressant in 104 patients. The RTX schedule comprised two injections (1 g, 2 weeks apart), repeated every 6 months until CR or failure, with a unique consolidation injection (1 g) after CR. The median survival times to disease control and to CR were 7.1 months and 12.2 months, respectively. The median number of RTX cycles required to achieve CR in 85.3% of patients was two. The larynx was the lesional site that took the longest time to achieve disease control. One year after RTX weaning, CR off RTX was obtained in 68.7% of cases. CR off RTX with only minimum doses of immunomodulatory drugs was achieved in 22.0% of patients. Further, 10.1% of patients were partial responders and 4.6% were non-responders to RTX. Relapse occurred in 38.7% of cases, of whom 91.7% had achieved CR again at the last follow-up. In MMP, CR was achieved in a longer time and after more rituximab cycles than in pemphigus, especially for patients with MMP with anti-type VII collagen reactivity. RTX with concomitant immunomodulatory drugs was not responsible for an unusual proportion of adverse events. This large study confirms that RTX is an effective therapy in patients with severe and/or refractory MMP, corroborating previous findings regarding the effects of RTX on AIBDs such as pemphigus.
Keywords: autoimmune bullous diseases; epidermolysis bullosa acquisita; fibrotic conjunctivitis; linear bullous IgA dermatosis; mucous membrane pemphigoid; rituximab.
Copyright © 2022 Bohelay, Alexandre, Le Roux-Villet, Sitbon, Doan, Soued, Shourick, Rousset, Mellottee, Heller, Lièvre, Zumelzu, Morin, Grootenboer-Mignot, Gabison, Caux, Prost-Squarcioni and Musette.
Conflict of interest statement
GB, MA, CL-V, FC, CP-P, and PM were investigators in the “Ritux 3” study (NCT00784589) and the “Pemphix” trial (NCT02383589) conducted by Roche Laboratories. MA, CL-V, FC, CP-P, and PM are investigators in “RTX-MMP” study (NCT03295383). The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Chan LS, Ahmed AR, Anhalt GJ, Bernauer W, Cooper KD, Elder MJ, et al. The First International Consensus on Mucous Membrane Pemphigoid: Definition, Diagnostic Criteria, Pathogenic Factors, Medical Treatment, and Prognostic Indicators. Arch Dermatol (2002) 138:370–9. doi: 10.1001/archderm.138.3.370 - DOI - PubMed
-
- Schmidt E, Rashid H, Marzano AV, Lamberts A, Di Zenzo G, Diercks GFH, et al. European Guidelines (S3) on Diagnosis and Management of Mucous Membrane Pemphigoid, Initiated by the European Academy of Dermatology and Venereology – Part Ii. J Eur Acad Dermatol Venereol (2021) 35:1926–48. doi: 10.1111/jdv.17395 - DOI - PMC - PubMed
-
- Rashid H, Lamberts A, Borradori L, Alberti-Violetti S, Barry RJ, Caproni M, et al. European Guidelines (S3) on Diagnosis and Management of Mucous Membrane Pemphigoid, Initiated by the European Academy of Dermatology and Venereology - Part I. J Eur Acad Dermatol Venereol (2021) 35:1750–64. doi: 10.1111/jdv.17397 - DOI - PMC - PubMed
-
- Gonzalez-Moles MA, Ruiz-Avila I, Rodriguez-Archilla A, Morales-Garcia P, Mesa-Aguado F, Bascones-Martinez A, et al. Treatment of Severe Erosive Gingival Lesions by Topical Application of Clobetasol Propionate in Custom Trays. Oral Surg Oral Med Oral Pathol Oral Radiol Endod (2003) 95:688–92. doi: 10.1067/moe.2003.139 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous