

Altered Balance of Pro-Inflammatory Immune Cells to T Regulatory Cells Differentiates Symptomatic From Asymptomatic Individuals With Anti-Nuclear Antibodies
- PMID: 35844549
- PMCID: PMC9279569
- DOI: 10.3389/fimmu.2022.886442
Altered Balance of Pro-Inflammatory Immune Cells to T Regulatory Cells Differentiates Symptomatic From Asymptomatic Individuals With Anti-Nuclear Antibodies
Abstract
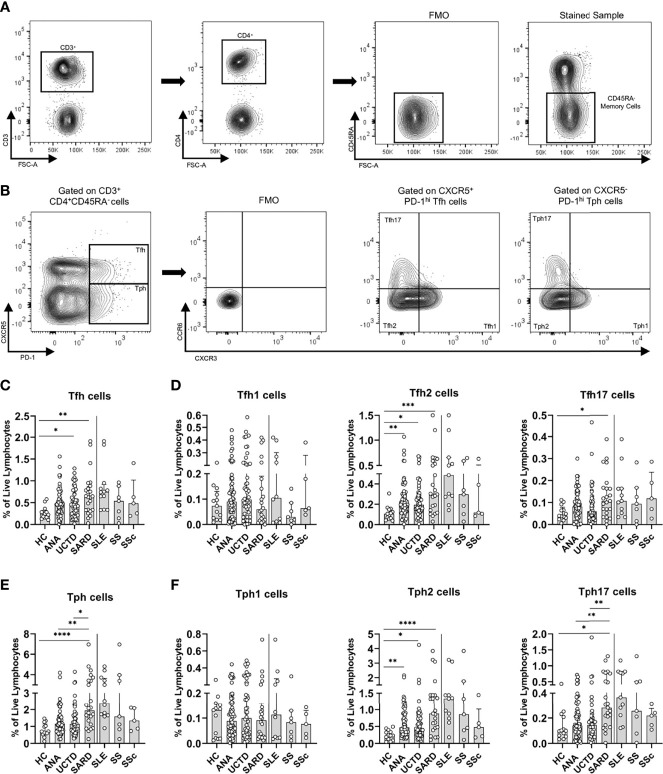
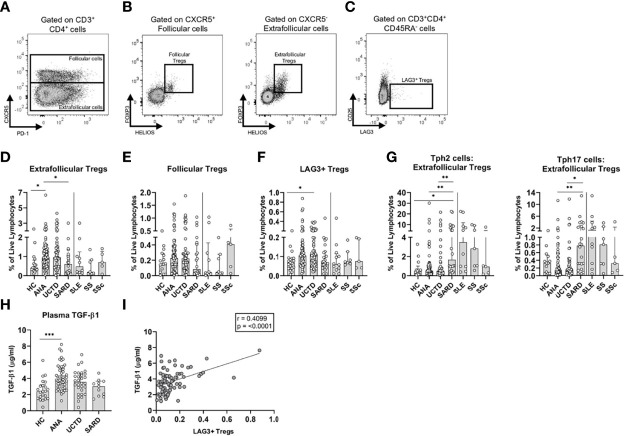
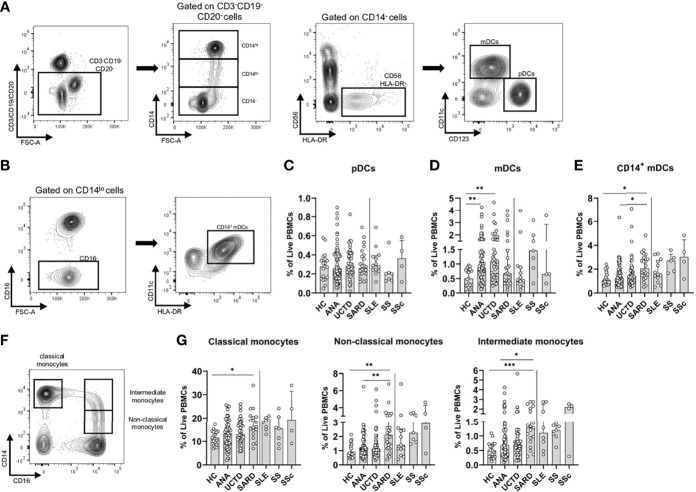
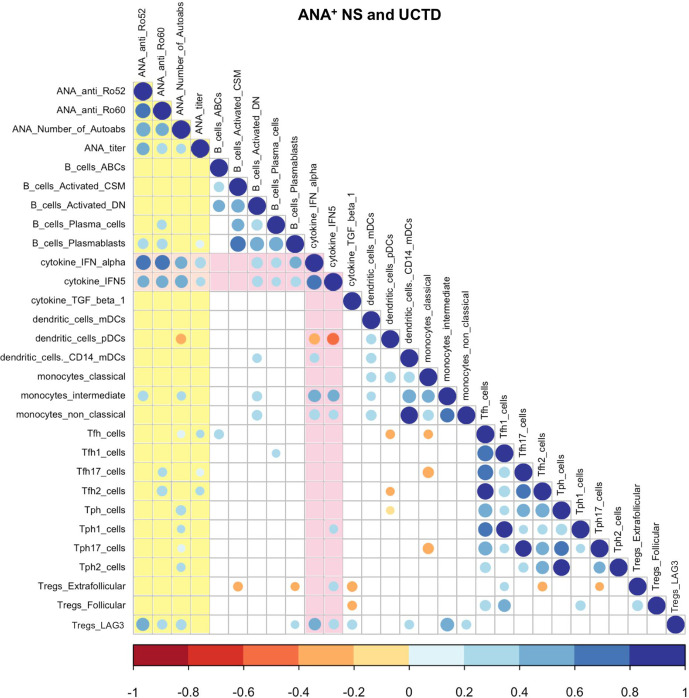
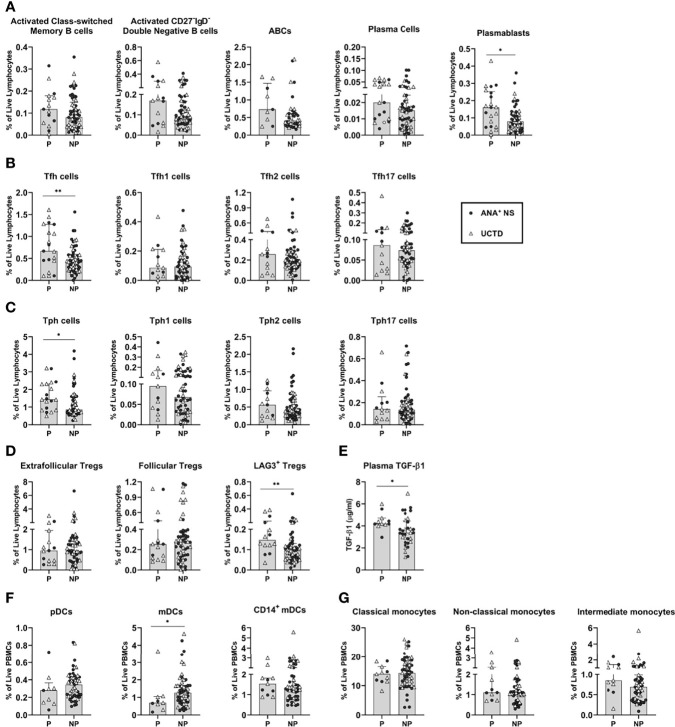
Systemic Autoimmune Rheumatic Diseases (SARDs) are characterized by the production of anti-nuclear antibodies (ANAs). ANAs are also seen in healthy individuals and can be detected years before disease onset in SARD. Both the immunological changes that promote development of clinical symptoms in SARD and those that prevent autoimmunity in asymptomatic ANA+ individuals (ANA+ NS) remain largely unexplored. To address this question, we used flow cytometry to examine peripheral blood immune populations in ANA+ individuals, with and without SARD, including 20 individuals who subsequently demonstrated symptom progression. Several immune populations were expanded in ANA+ individuals with and without SARD, as compared with ANA- healthy controls, particularly follicular and peripheral T helper, and antibody-producing B cell subsets. In ANA+ NS individuals, there were significant increases in T regulatory subsets and TGF-ß1 that normalized in SARD patients, whereas in SARD patients there were increases in Th2 and Th17 helper cell levels as compared with ANA+ NS individuals, resulting in a shift in the balance between inflammatory and regulatory T cell subsets. Patients with SARD also had increases in the proportion of pro-inflammatory innate immune cell populations, such as CD14+ myeloid dendritic cells, and intermediate and non-classical monocytes, as compared to ANA+ NS individuals. When comparing ANA+ individuals without SARD who progressed clinically over the subsequent 2 years with those who did not, we found that progressors had significantly increased T and B cell activation, as well as increased levels of LAG3+ T regulatory cells and TGF-ß1. Collectively, our findings suggest that active immunoregulation prevents clinical autoimmunity in ANA+ NS and that this becomes impaired in patients who progress to SARD, resulting in an imbalance favoring inflammation.
Keywords: anti-nuclear antibodies; b cells; dendritic cells; interferon-alpha; monocytes; systemic autoimmune rheumatic diseases; t cells; t regulatory cells.
Copyright © 2022 Gupta, Vanlieshout, Manion, Bonilla, Kim, Muñoz-Grajales, Nassar, Johnson, Hiraki, Ahmad, Touma, Bookman and Wither.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The presence of anti-nuclear antibodies alone is associated with changes in B cell activation and T follicular helper cells similar to those in systemic autoimmune rheumatic disease.Arthritis Res Ther. 2018 Nov 29;20(1):264. doi: 10.1186/s13075-018-1752-3. Arthritis Res Ther. 2018. PMID: 30486869 Free PMC article.
-
Presence of an interferon signature in individuals who are anti-nuclear antibody positive lacking a systemic autoimmune rheumatic disease diagnosis.Arthritis Res Ther. 2017 Feb 28;19(1):41. doi: 10.1186/s13075-017-1243-y. Arthritis Res Ther. 2017. PMID: 28245862 Free PMC article.
-
Interferon and interferon-induced cytokines as markers of impending clinical progression in ANA+ individuals without a systemic autoimmune rheumatic disease diagnosis.Arthritis Res Ther. 2023 Feb 10;25(1):21. doi: 10.1186/s13075-023-02997-w. Arthritis Res Ther. 2023. PMID: 36765391 Free PMC article.
-
Autoantibodies Against DFS70/LEDGF Exclusion Markers for Systemic Autoimmune Rheumatic Diseases (SARD).Clin Lab. 2016;62(4):499-517. doi: 10.7754/clin.lab.2015.150905. Clin Lab. 2016. PMID: 27215068 Review.
-
Importance of the dense fine speckled pattern on HEp-2 cells and anti-DFS70 antibodies for the diagnosis of systemic autoimmune diseases.Autoimmun Rev. 2012 Jul;11(9):642-5. doi: 10.1016/j.autrev.2011.11.005. Epub 2011 Nov 11. Autoimmun Rev. 2012. PMID: 22100330 Review.
Cited by
-
Advanced Autoantibody Testing in Systemic Sclerosis.Diagnostics (Basel). 2023 Feb 23;13(5):851. doi: 10.3390/diagnostics13050851. Diagnostics (Basel). 2023. PMID: 36899995 Free PMC article. Review.
-
Evaluation of Progression From Preclinical to Systemic Autoimmune Rheumatic Disease: Novel Use of the European Alliance of Associations for Rheumatology/American College of Rheumatology Systemic Lupus Erythematosus Classification Criteria as an Outcome Measure.ACR Open Rheumatol. 2024 Dec;6(12):871-877. doi: 10.1002/acr2.11723. Epub 2024 Sep 30. ACR Open Rheumatol. 2024. PMID: 39348240 Free PMC article.
References
-
- Bentham J, Morris DL, Cunninghame Graham DS, Pinder CL, Tombleson P, Behrens TW, et al. . Genetic Association Analyses Implicate Aberrant Regulation of Innate and Adaptive Immunity Genes in the Pathogenesis of Systemic Lupus Erythematosus. Nat Genet (2015) 47(12):1457–64. doi: 10.1038/ng.3434 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous