

Association Between the Use of Pre- and Post-thrombolysis Anticoagulation With All-Cause Mortality and Major Bleeding in Patients With Pulmonary Embolism
- PMID: 35845061
- PMCID: PMC9279684
- DOI: 10.3389/fcvm.2022.880189
Association Between the Use of Pre- and Post-thrombolysis Anticoagulation With All-Cause Mortality and Major Bleeding in Patients With Pulmonary Embolism
Abstract
Objective: To explore the comparative clinical efficacy and safety outcomes of anticoagulation before (pre-) or following (post-) thrombolytic therapy in systemic thrombolytic therapy for pulmonary embolism (PE).
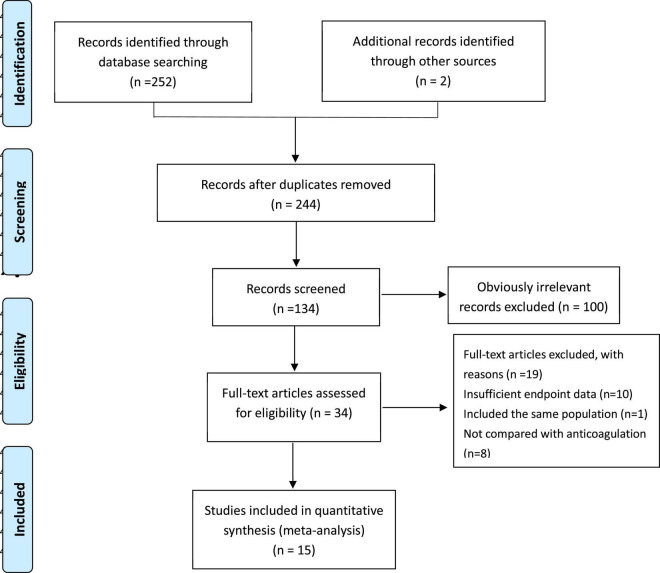
Methods: PubMed, the Cochrane Library, EMBASE, EBSCO, Web of Science, and CINAHL databases were searched from inception through 1 May 2021. All randomized clinical trials comparing systemic thrombolytic therapy vs. anticoagulation alone in patients with PE and those that were written in English were eligible. The primary efficacy and safety outcomes were all-cause mortality and major bleeding, respectively. Odds ratios (OR) estimates and associated 95% confidence intervals (CIs) were calculated. A Bayesian network analysis was performed using R studio software, and then the efficacy and safety rankings were derived.
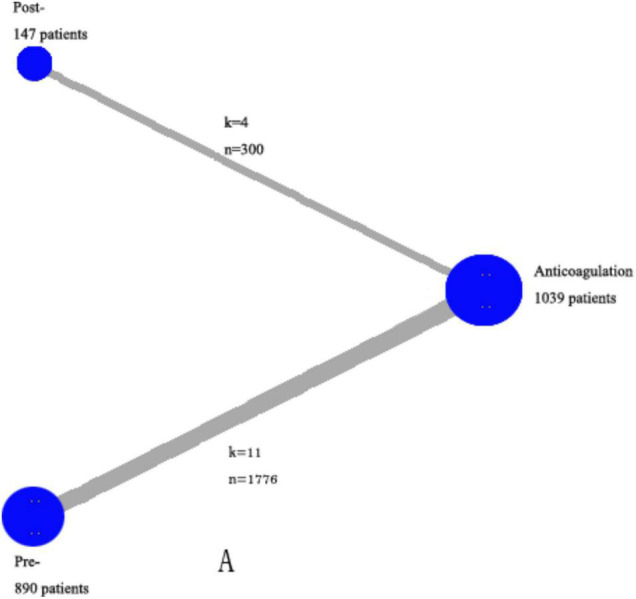
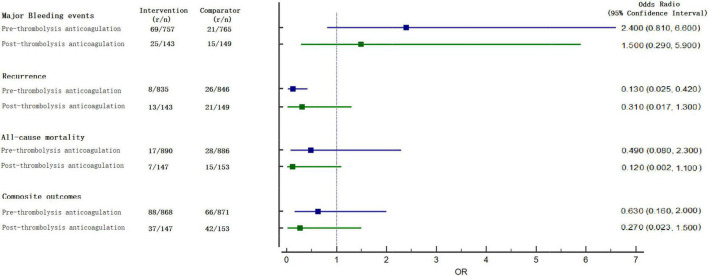
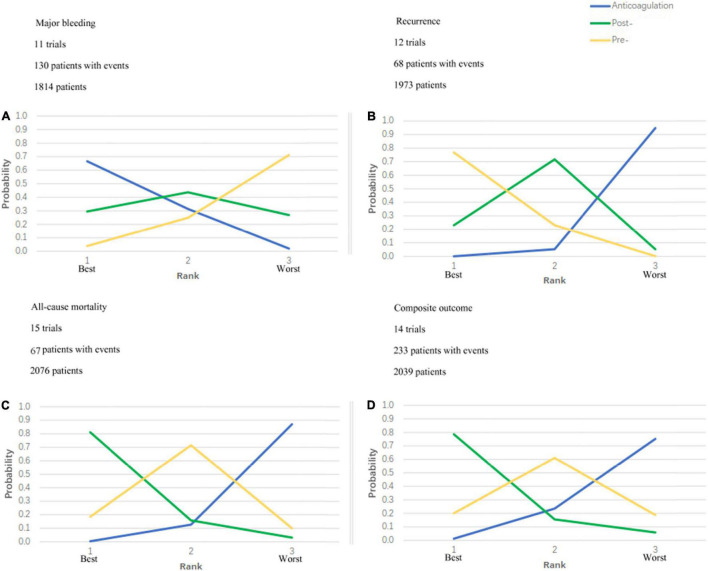
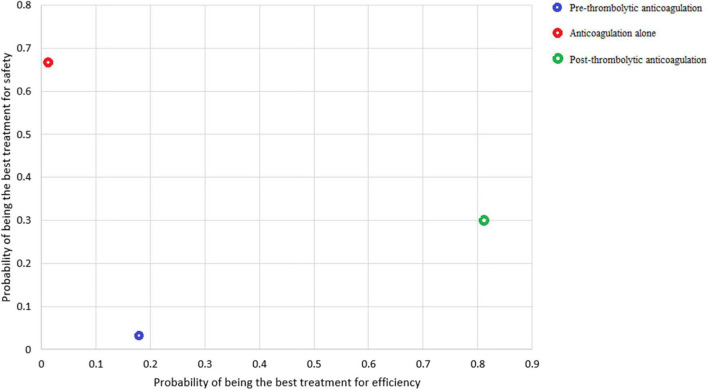
Results: This network meta-analysis enrolled 15 trials randomizing 2,076 patients. According to the plot rankings, the anticoagulant therapy was the best in terms of major bleeding, and the post-thrombolysis anticoagulation was the best in terms of all-cause mortality. Taking major bleeding and all-cause mortality into consideration, the most safe-effective treatment was the post-thrombolysis anticoagulation in patients who needed thrombolytic therapy. The net clinical benefit analysis comparing associated ICH benefits vs. mortality risks of post-thrombolysis anticoagulation demonstrated a net clinical benefit of 1.74%.
Conclusion: The systemic thrombolysis followed by anticoagulation had a better advantage in all-cause mortality and major bleeding than the systemic thrombolysis before anticoagulation. The adjuvant anticoagulation treatment of systemic thrombolytic therapy should be optimized.
Keywords: all-cause mortality; anticoagulation (AC); major bleeding; pulmonary embolism; thrombolysis/thrombolytic agents.
Copyright © 2022 Tan, Liu, Hu, Wu, Gao, Guo, Yan, Peng and Hua.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis.JAMA. 2014 Jun 18;311(23):2414-21. doi: 10.1001/jama.2014.5990. JAMA. 2014. PMID: 24938564
-
Thrombolysis for acute intermediate-risk pulmonary embolism: A meta-analysis.Thromb Res. 2015 Nov;136(5):932-7. doi: 10.1016/j.thromres.2015.09.012. Epub 2015 Sep 12. Thromb Res. 2015. PMID: 26384442
-
Comparison of Efficacy and Safety between Thrombolysis Plus Anticoagulation vs. Anticoagulation Alone for the Treatment of Acute Submassive Pulmonary Embolism: A Systematic Review and Meta-analysis.Curr Vasc Pharmacol. 2022;20(6):491-500. doi: 10.2174/1570161120666220811155353. Curr Vasc Pharmacol. 2022. PMID: 35959626
-
Initial thrombolysis treatment compared with anticoagulation for acute intermediate-risk pulmonary embolism: a meta-analysis.J Thorac Dis. 2015 May;7(5):810-21. doi: 10.3978/j.issn.2072-1439.2015.04.51. J Thorac Dis. 2015. PMID: 26101636 Free PMC article.
-
Thrombolysis versus anticoagulation for the initial treatment of moderate pulmonary embolism: a meta-analysis of randomized controlled trials.Respir Care. 2014 Dec;59(12):1880-7. doi: 10.4187/respcare.03197. Epub 2014 Sep 30. Respir Care. 2014. PMID: 25269681 Review.
Cited by
-
Clinical and Safety Outcomes Associated with Extended Treatment of Venous Thromboembolism: A Network Meta-Analysis.J Cardiovasc Dev Dis. 2022 Nov 25;9(12):414. doi: 10.3390/jcdd9120414. J Cardiovasc Dev Dis. 2022. PMID: 36547411 Free PMC article. Review.
References
-
- Chatterjee S, Chakraborty A, Weinbe0rg I, Kadakia M, Wilensky RL, Sardar P, et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. (2014) 311:2414–21. - PubMed
-
- Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser K, Rauber K, et al. Association between thrombolytic treatment and the prognosis of hemodynamically stable patients with major pulmonary embolism: results of a multicenter registry. Circulation. (1997) 96:882–8. 10.1161/01.cir.96.3.882 - DOI - PubMed
-
- Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. (2016) 149:315–52. - PubMed
Publication types
LinkOut - more resources
Full Text Sources