

A prediction model with measured sentiment scores for the risk of in-hospital mortality in acute pancreatitis: a retrospective cohort study
- PMID: 35845515
- PMCID: PMC9279801
- DOI: 10.21037/atm-22-1613
A prediction model with measured sentiment scores for the risk of in-hospital mortality in acute pancreatitis: a retrospective cohort study
Abstract
Background: Accurate and prompt clinical assessment of the severity and prognosis of patients with acute pancreatitis (AP) is critical, particularly during hospitalization. Natural language processing algorithms gain an opportunity from the growing number of free-text notes in electronic health records to mine this unstructured data, e.g., nursing notes, to detect and predict adverse outcomes. However, the predictive value of nursing notes for AP prognosis is unclear. In this study, a predictive model for in-hospital mortality in AP was developed using measured sentiment scores in nursing notes.
Methods: The data of AP patients in the retrospective cohort study were collected from the Medical Information Mart for Intensive Care III (MIMIC-III) database. Sentiments in nursing notes were assessed by sentiment analysis. For each individual clinical note, sentiment polarity and sentiment subjectivity scores were assigned. The in-hospital mortality of AP patients was the outcome. A predictive model was built based on clinical information and sentiment scores, and its performance and clinical value were evaluated using the area under curves (AUCs) and decision-making curves, respectively.
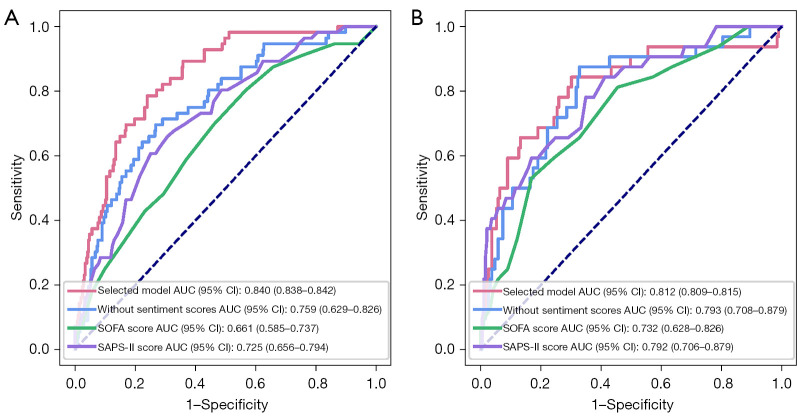
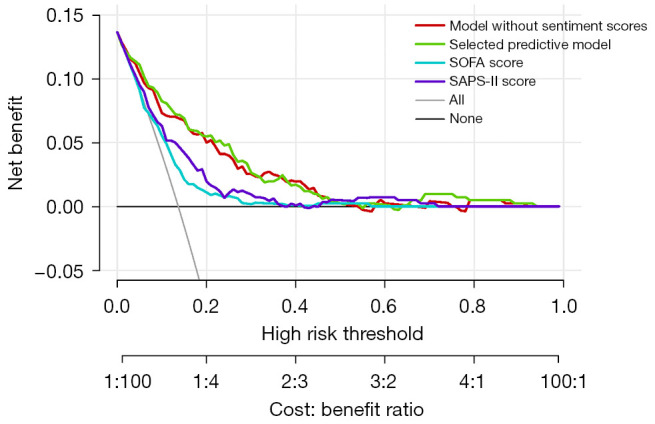
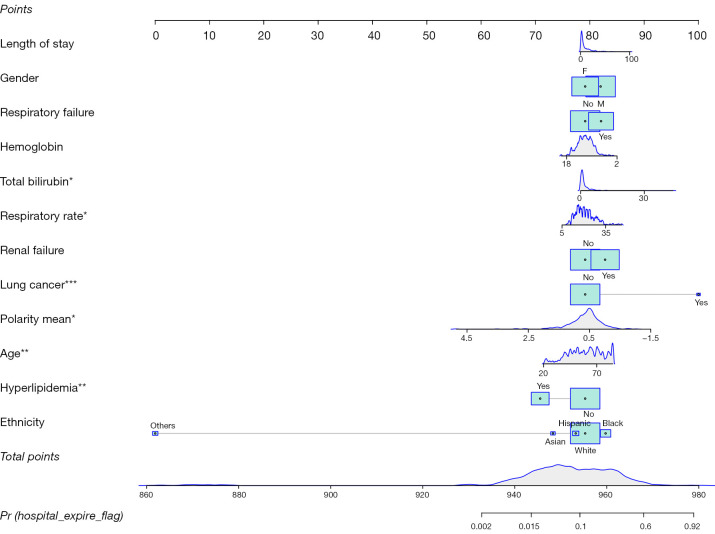
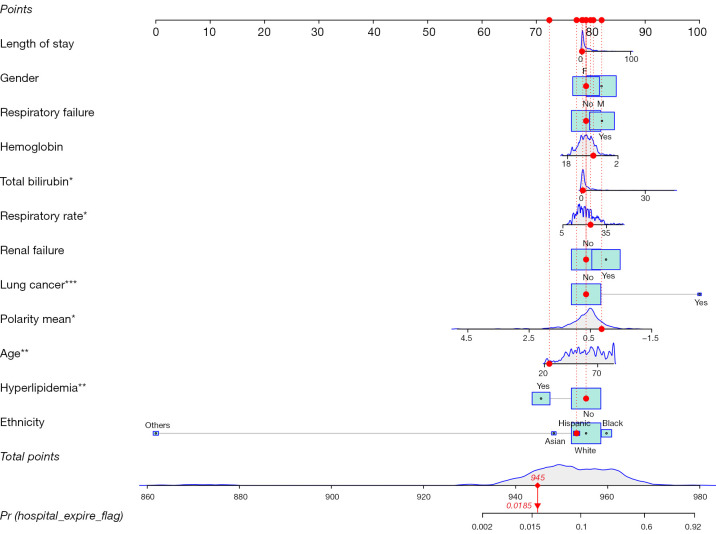
Results: Of the 631 AP patients included, 88 cases (13.9%) cases were dead in hospital. When various confounding factors were adjusted, the mean sentiment polarity was associated with a reduced risk of in-hospital mortality in AP [odds ratio (OR): 0.448; 95% confidence interval (CI): 0.233-0.833; P=0.014]. A predictive model was established in the training group via multivariate logistic regression analysis, including 12 independent variables. In the testing group, the model showed an AUC of 0.812, which was significantly greater than the sequential organ failure assessment (SOFA) of 0.732 and the simplified acute physiology score-II (SAPS-II) of 0.792 (P<0.05). When the same level of risk was considered, the clinical benefits of the predictive model were found to be the highest compared with SOFA and SAPS-II scores.
Conclusions: The model combined sentiment scores in nursing notes showed well predictive performance and clinical value in in-hospital mortality of AP patients.
Keywords: Acute pancreatitis; Medical Information Mart for Intensive Care III (MIMIC-III); in-hospital mortality; predictive model; sentiment.
2022 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-1613/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Sentiment Analysis Based on the Nursing Notes on In-Hospital 28-Day Mortality of Sepsis Patients Utilizing the MIMIC-III Database.Comput Math Methods Med. 2021 Oct 13;2021:3440778. doi: 10.1155/2021/3440778. eCollection 2021. Comput Math Methods Med. 2021. PMID: 34691236 Free PMC article.
-
Sentiment in nursing notes as an indicator of out-of-hospital mortality in intensive care patients.PLoS One. 2018 Jun 7;13(6):e0198687. doi: 10.1371/journal.pone.0198687. eCollection 2018. PLoS One. 2018. PMID: 29879201 Free PMC article.
-
Sentiment Analysis for Necessary Preview of 30-Day Mortality in Sepsis Patients and the Control Strategies.J Healthc Eng. 2021 Oct 25;2021:1713363. doi: 10.1155/2021/1713363. eCollection 2021. J Healthc Eng. 2021. PMID: 34733452 Free PMC article.
-
Construction and validation of machine learning models for sepsis prediction in patients with acute pancreatitis.BMC Surg. 2023 Sep 1;23(1):267. doi: 10.1186/s12893-023-02151-y. BMC Surg. 2023. PMID: 37658375 Free PMC article. Clinical Trial.
-
Performance of Sequential Organ Failure Assessment and Simplified Acute Physiology Score II for Post-Cardiac Surgery Patients in Intensive Care Unit.Front Cardiovasc Med. 2021 Dec 6;8:774935. doi: 10.3389/fcvm.2021.774935. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34938790 Free PMC article.
Cited by
-
Natural language processing in the intensive care unit: A scoping review.Crit Care Resusc. 2024 Jul 31;26(3):210-216. doi: 10.1016/j.ccrj.2024.06.008. eCollection 2024 Sep. Crit Care Resusc. 2024. PMID: 39355491 Free PMC article.
-
Development and Validation of a Dynamic Nomogram for Predicting in-Hospital Mortality in Patients with Acute Pancreatitis: A Retrospective Cohort Study in the Intensive Care Unit.Int J Gen Med. 2023 Jun 17;16:2541-2553. doi: 10.2147/IJGM.S409812. eCollection 2023. Int J Gen Med. 2023. PMID: 37351008 Free PMC article.
-
Construction and validation of a nomogram for predicting survival in elderly patients with severe acute pancreatitis: a retrospective study from a tertiary center.BMC Gastroenterol. 2024 Jul 8;24(1):219. doi: 10.1186/s12876-024-03308-6. BMC Gastroenterol. 2024. PMID: 38977953 Free PMC article.
-
Construction and validation of a nomogram for predicting survival in diabetic patients with severe acute pancreatitis: A retrospective study from a tertiary center.Saudi J Gastroenterol. 2025 Mar 1;31(2):68-74. doi: 10.4103/sjg.sjg_178_24. Epub 2025 Feb 7. Saudi J Gastroenterol. 2025. PMID: 39918039 Free PMC article.
-
Chronic liver disease is an important risk factor for worse outcomes in acute pancreatitis: a systematic review and meta-analysis.Sci Rep. 2024 Jul 19;14(1):16723. doi: 10.1038/s41598-024-66710-w. Sci Rep. 2024. PMID: 39030187 Free PMC article.
References
LinkOut - more resources
Full Text Sources