

Bacillary layer detachment in serpiginous-like choroiditis of presumed intraocular tuberculosis: Report of two cases
- PMID: 35845750
- PMCID: PMC9278036
- DOI: 10.1016/j.ajoc.2022.101653
Bacillary layer detachment in serpiginous-like choroiditis of presumed intraocular tuberculosis: Report of two cases
Abstract
Purpose: To describe the presence of bacillary layer detachment (BALAD) in serpiginous-like choroiditis (SLC) in presumed intraocular tuberculosis.
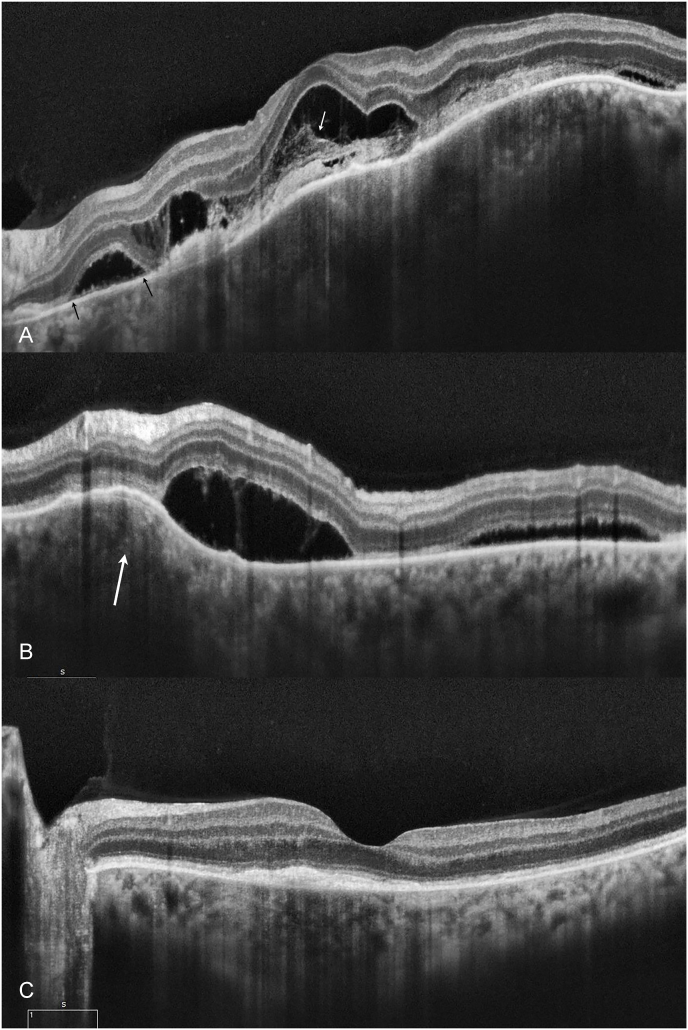
Observations: Clinical and multimodal imaging including fundus photography, fundus autofluorescence, and spectral domain and enhanced-deep imaging optical coherence tomography (OCT) of two cases of SLC in presumed intraocular tuberculosis. Two patients (26 and 38-year-old woman) presented with unilateral, decreased vision of acute onset. They were diagnosed with SLC in presumed intraocular tuberculosis, and OCT revealed splitting of the ellipsoid zone, resembling BALAD. All two patients showed complete resolution after treatment with antitubercular therapy (ATT).
Conclusions and importance: BALAD appears in the acute stage of SLC in presumed intraocular tuberculosis and resolves rapidly at the beginning of ATT.
Keywords: Bacillary layer detachment; Optical coherence tomography; Photoreceptor layer; Serpiginous-like choroiditis; Tuberculosis; Uveitis.
© 2022 Published by Elsevier Inc.
Conflict of interest statement
The following authors have no financial disclosures: da Costa D.S.; Silva A. G., Melichar A., Neves D. B., Correa P. A., Moraes R. T.
Figures





References
-
- WHO . World Health Organization; Geneva: 2020. Global Tuberculosis Report 2020. Licence: CC BY-NC-SA 3.0 IGO.
-
- Gupta A., Bansal R., Gupta V., Sharma A., Bambery P. Ocular signs predictive of tubercular uveitis. Am J Ophthalmol. 2010;149:562–570. - PubMed
-
- Kawali A., Bavaharan B., Sanjay S., et al. Serpiginous-like choroiditis (SLC) –Morphology and treatment outcomes. Ocul Immunol Inflamm. 2019:1–9. 0(0) - PubMed
-
- Kohli G.M., Bhatia P., Sen A., Gupta A. Bacillary layer detachment in hyper-acute stage of acute posterior multifocal placoid pigment epitheliopathy: a case series. Ocul Immunol Inflamm. 2020 Sep;23:1–4. - PubMed
-
- Cicinelli MV, Giuffré C, Marchese A, et al. The bacillary detachment in posterior segment ocular diseases. Am Acad Opthalmol. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
