

A Novel Composite Indicator of Predicting Mortality Risk for Heart Failure Patients With Diabetes Admitted to Intensive Care Unit Based on Machine Learning
- PMID: 35846312
- PMCID: PMC9277005
- DOI: 10.3389/fendo.2022.917838
A Novel Composite Indicator of Predicting Mortality Risk for Heart Failure Patients With Diabetes Admitted to Intensive Care Unit Based on Machine Learning
Abstract
Background: Patients with heart failure (HF) with diabetes may face a poorer prognosis and higher mortality than patients with either disease alone, especially for those in intensive care unit. So far, there is no precise mortality risk prediction indicator for this kind of patient.
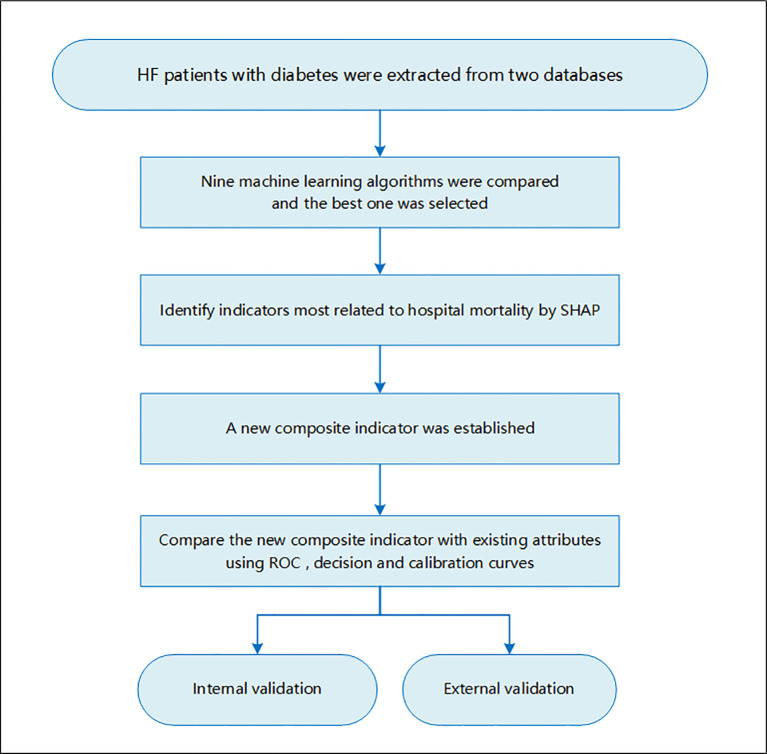
Method: Two high-quality critically ill databases, the Medical Information Mart for Intensive Care IV (MIMIC-IV) database and the Telehealth Intensive Care Unit (eICU) Collaborative Research Database (eICU-CRD) Collaborative Research Database, were used for study participants' screening as well as internal and external validation. Nine machine learning models were compared, and the best one was selected to define indicators associated with hospital mortality for patients with HF with diabetes. Existing attributes most related to hospital mortality were identified using a visualization method developed for machine learning, namely, Shapley Additive Explanations (SHAP) method. A new composite indicator ASL was established using logistics regression for patients with HF with diabetes based on major existing indicators. Then, the new index was compared with existing indicators to confirm its discrimination ability and clinical value using the receiver operating characteristic (ROC) curve, decision curve, and calibration curve.
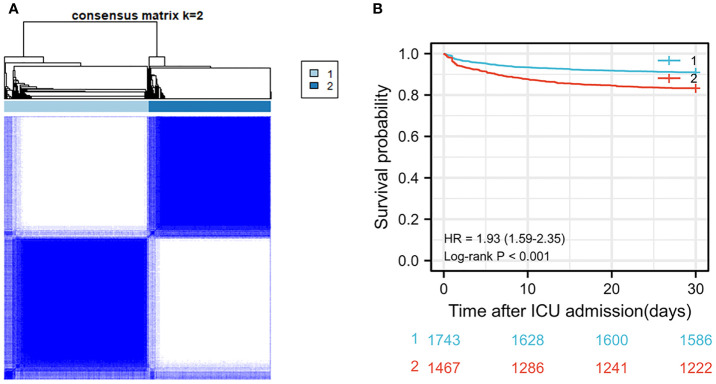
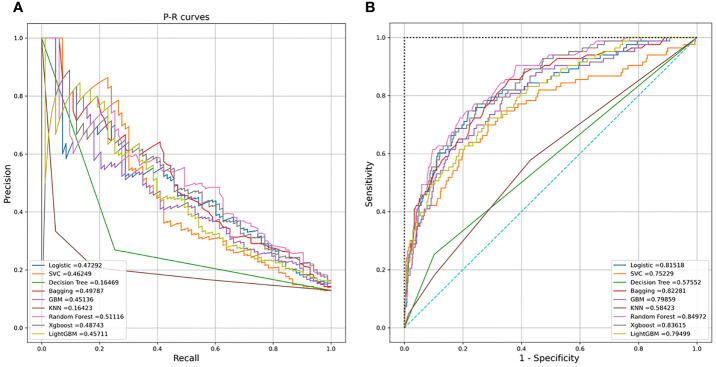
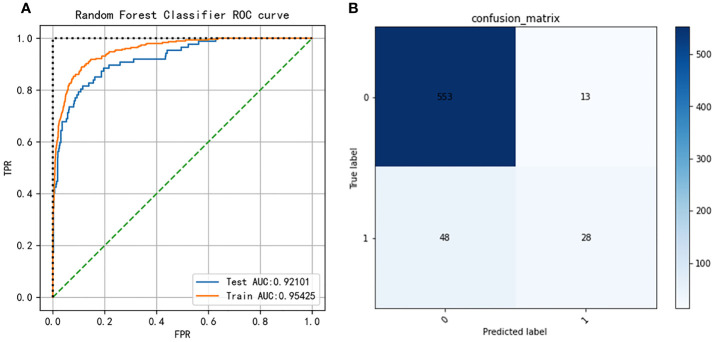
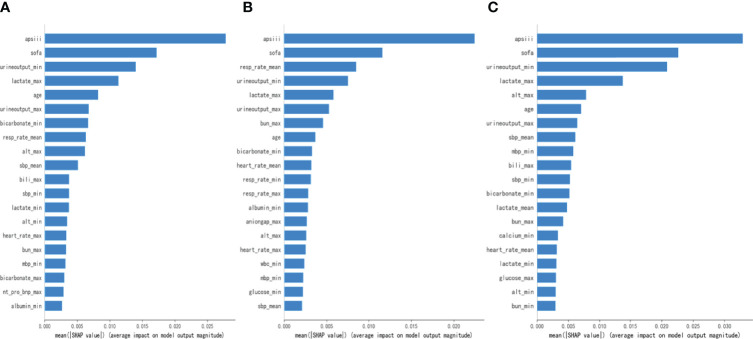
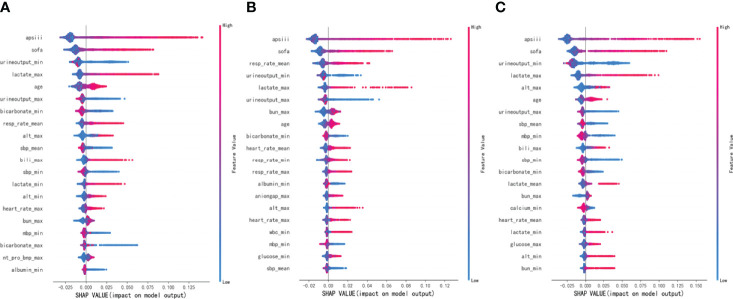
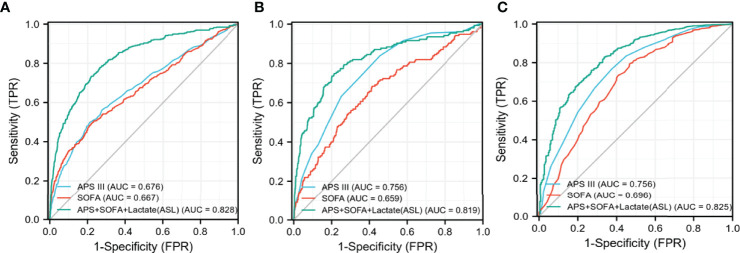
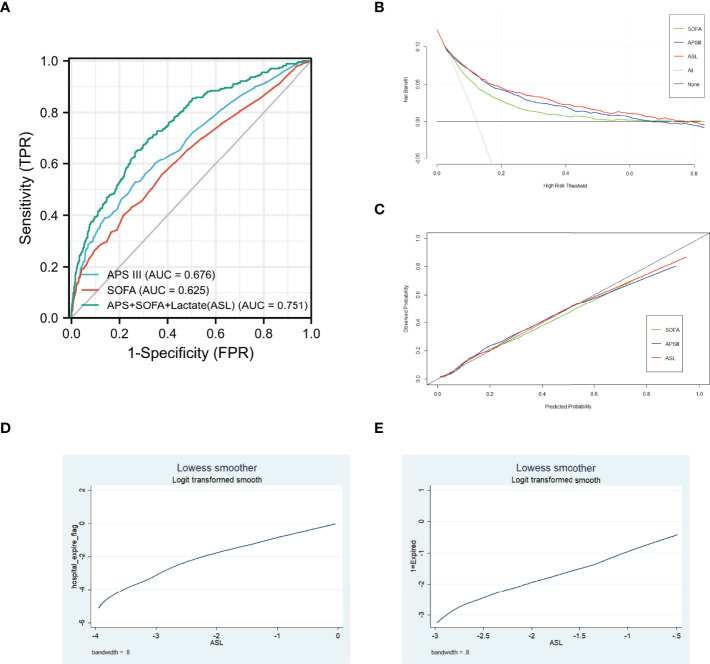
Results: The random forest model outperformed among nine models with the area under the ROC curve (AUC) = 0.92 after hyper-parameter optimization. By using this model, the top 20 attributes associated with hospital mortality in these patients were identified among all the attributes based on SHAP method. Acute Physiology Score (APS) III, Sepsis-related Organ Failure Assessment (SOFA), and Max lactate were selected as major attributes related to mortality risk, and a new composite indicator was developed by combining these three indicators, which was named as ASL. Both in the initial and external cohort, the new indicator, ASL, had greater risk discrimination ability with AUC higher than 0.80 in both low- and high-risk groups compared with existing attributes. The decision curve and calibration curve indicated that this indicator also had a respectable clinical value compared with APS III and SOFA. In addition, this indicator had a good risk stratification ability when the patients were divided into three risk levels.
Conclusion: A new composite indicator for predicting mortality risk in patients with HF with diabetes admitted to intensive care unit was developed on the basis of attributes identified by the random forest model. Compared with existing attributes such as APS III and SOFA, the new indicator had better discrimination ability and clinical value, which had potential value in reducing the mortality risk of these patients.
Keywords: diabetes; heart failure; hospital mortality; indicator; machine learning.
Copyright © 2022 Yang, Zhu, Lu and Shen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases.Front Cardiovasc Med. 2022 Oct 12;9:994359. doi: 10.3389/fcvm.2022.994359. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312291 Free PMC article.
-
Machine learning-based in-hospital mortality risk prediction tool for intensive care unit patients with heart failure.Front Cardiovasc Med. 2023 Apr 3;10:1119699. doi: 10.3389/fcvm.2023.1119699. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37077747 Free PMC article.
-
The prediction of in-hospital mortality in chronic kidney disease patients with coronary artery disease using machine learning models.Eur J Med Res. 2023 Jan 18;28(1):33. doi: 10.1186/s40001-023-00995-x. Eur J Med Res. 2023. PMID: 36653875 Free PMC article.
-
Predicting Acute Onset of Heart Failure Complicating Acute Coronary Syndrome: An Explainable Machine Learning Approach.Curr Probl Cardiol. 2023 Feb;48(2):101480. doi: 10.1016/j.cpcardiol.2022.101480. Epub 2022 Nov 3. Curr Probl Cardiol. 2023. PMID: 36336116 Review.
-
Machine learning for the prediction of sepsis-related death: a systematic review and meta-analysis.BMC Med Inform Decis Mak. 2023 Dec 11;23(1):283. doi: 10.1186/s12911-023-02383-1. BMC Med Inform Decis Mak. 2023. PMID: 38082381 Free PMC article.
Cited by
-
The predictive value of SOFA and APSIII scores for 28-day mortality risk in SIMI: a cohort study based on the MIMIC-IV database.Front Cell Infect Microbiol. 2025 Jul 29;15:1574625. doi: 10.3389/fcimb.2025.1574625. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40799939 Free PMC article.
-
Machine learning for risk prediction of acute kidney injury in patients with diabetes mellitus combined with heart failure during hospitalization.Sci Rep. 2025 Mar 28;15(1):10728. doi: 10.1038/s41598-025-87268-1. Sci Rep. 2025. PMID: 40155666 Free PMC article.
-
Predictive Value of Machine Learning for the Risk of In-Hospital Death in Patients With Heart Failure: A Systematic Review and Meta-Analysis.Clin Cardiol. 2025 Jan;48(1):e70071. doi: 10.1002/clc.70071. Clin Cardiol. 2025. PMID: 39723651 Free PMC article.
-
Predicting Successful Weaning from Mechanical Ventilation by Reduction in Positive End-expiratory Pressure Level Using Machine Learning.PLOS Digit Health. 2024 Mar 27;3(3):e0000478. doi: 10.1371/journal.pdig.0000478. eCollection 2024 Mar. PLOS Digit Health. 2024. PMID: 38536802 Free PMC article.
-
Prediction of 30-day mortality in heart failure patients with hypoxic hepatitis: Development and external validation of an interpretable machine learning model.Front Cardiovasc Med. 2022 Oct 28;9:1035675. doi: 10.3389/fcvm.2022.1035675. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36386374 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous